
Retinal vasculitis means inflammation affecting the blood vessels of the retina, the light-sensitive tissue at the back of the eye. Patients often worry most when they hear about bleeding, scarring, blocked vessels, or macular edema, because these problems can reduce vision and may change treatment urgency. The key point is that treatment is no longer just about “quieting inflammation.” Doctors also look for infection, vessel blockage, retinal ischemia, and swelling in the macula. The more retinal damage there is, the more closely treatment, imaging, and follow-up usually need to be tailored.
Retinal Vasculitis and Macular Edema: The Complications Patients Mention Most—and How Treatment Paths Change
When patients are told they have retinal vasculitis, the first reaction is often confusion. The second is usually fear. Many people have never heard the term before. Then, during scans or follow-up visits, they may hear other alarming words: hemorrhage, scarring, ischemia, leakage, cystoid macular edema, or neovascularization. These are the terms patients tend to remember because they sound serious, and often they are.
From a doctor’s point of view, that concern is understandable. Retinal vasculitis is not just “eye inflammation.” It is inflammation involving the retinal blood vessels, and the retina is one of the most important parts of the eye for vision. When blood vessels become inflamed, they can leak, close off, bleed, or trigger damage in surrounding retinal tissue. That is why retinal involvement often changes both prognosis and treatment planning. (PMC)
To understand why treatment paths change, it helps to start with one basic idea: retinal vasculitis is not one single disease. It is a clinical finding. It can happen with non-infectious uveitis, autoimmune disease, Behçet disease, sarcoidosis, lupus, multiple sclerosis, tuberculosis, syphilis, viral infections, and other conditions. In some patients, no clear cause is found even after a careful workup. Because the causes vary so much, the “right” treatment is not the same for every patient. (PMC)
Why retinal involvement worries doctors more
Inflammation in the front part of the eye can be painful and dramatic, but retinal vasculitis is often more threatening to long-term vision because it affects the tissue responsible for detailed sight. Inflammation around retinal vessels can lead to leakage, retinal swelling, and reduced oxygen supply to the retina. If enough damage occurs, the eye can develop macular edema, areas of capillary nonperfusion, retinal ischemia, abnormal new vessels, vitreous hemorrhage, or permanent scarring. These are the complications that most strongly influence prognosis. (PMC)
Patients usually ask a very practical question: “Does this mean I’m going to lose vision?” The honest answer is that some people recover well, especially when inflammation is found early and treated properly. But vision risk rises when the macula is involved, when vessel closure causes ischemia, when bleeding obscures the retina, or when scarring affects central retinal tissue. That is why retinal vasculitis usually leads to closer monitoring than milder forms of eye inflammation. (NCBI)
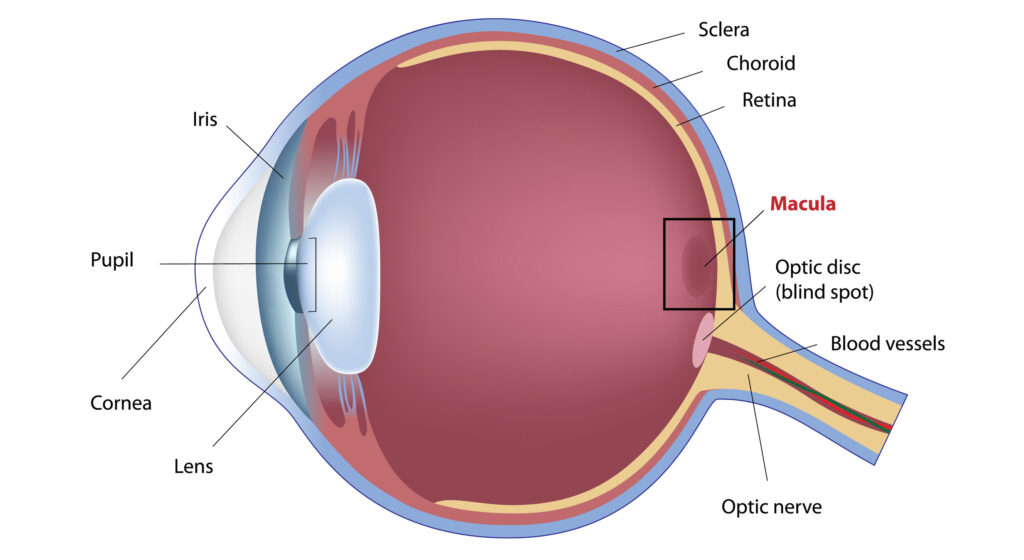
What the retina and macula actually do
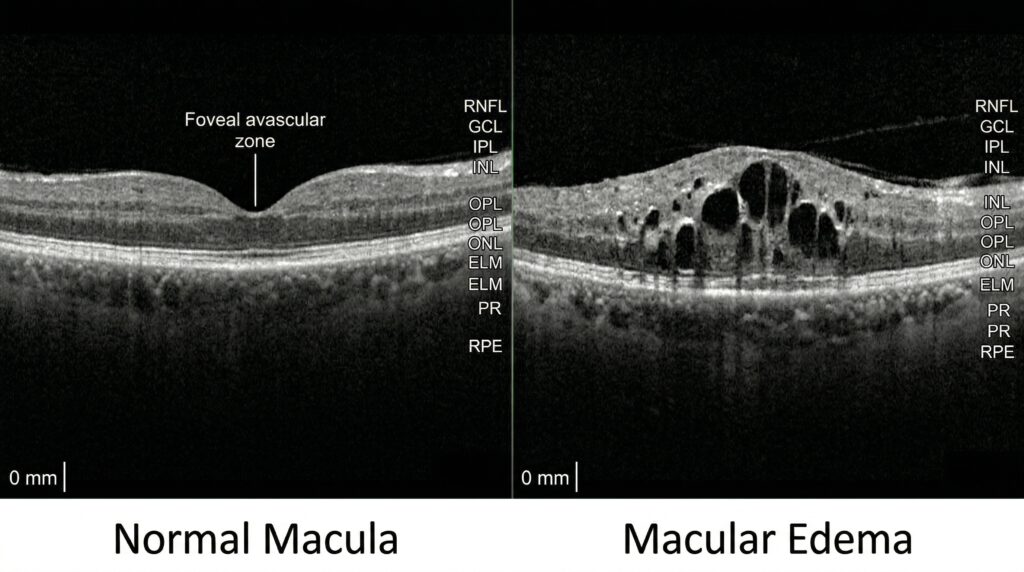
The retina lines the back of the eye and converts light into signals for the brain. The macula is the small central area of the retina responsible for reading vision, facial recognition, and fine detail. If the macula swells, even a relatively small amount, patients may notice blur, distortion, washed-out colors, or difficulty focusing on words. That is why macular edema often becomes the symptom patients mention most, even more than the vasculitis itself. (American Academy of Ophthalmology)
Macular edema simply means fluid buildup in the macula. In inflammatory eye disease, that fluid collects because inflammation disrupts the normal blood-retinal barrier. Blood vessels become leaky. Fluid and proteins escape into the retinal tissue. If that swelling persists, it can damage the retinal architecture and lead to lasting visual loss. In uveitis, macular edema is one of the leading causes of reduced vision. (American Academy of Ophthalmology)
The complications patients mention most
Patients with retinal vasculitis often talk about four findings again and again: macular edema, scarring, hemorrhages, and blocked blood vessels. These matter because they often signal that the disease is affecting the retina more deeply than surface inflammation alone. (PMC)
Macular edema: the complication that most often changes symptoms
Macular edema is often the reason a patient first realizes the disease is affecting vision in a meaningful way. A patient may say, “My vision is blurry in the center,” or “Straight lines look bent,” or “I can see, but nothing looks crisp.” That is very different from mild irritation or redness. When the macula swells, reading and driving can become difficult, even if the rest of the eye looks relatively quiet from the outside. (American Academy of Ophthalmology)
This matters because treatment goals change. In a patient with active retinal vasculitis and no macular edema, the main objective may be to suppress inflammation and prevent further vessel damage. In a patient with macular edema, the doctor must also actively reduce retinal swelling and protect central vision. That often means more frequent OCT scans, a lower threshold to escalate anti-inflammatory treatment, and sometimes local steroid therapy if appropriate. (NCBI)
Retinal hemorrhages: a sign that leakage or vessel damage is occurring
Hemorrhages are bleeding spots in or around the retina. They may be small and only seen on examination, or they may be larger and affect vision if bleeding extends into the vitreous cavity. Patients understandably become alarmed when they hear there is “bleeding in the eye.” In retinal vasculitis, hemorrhages can occur because inflamed vessels become damaged, fragile, or blocked. They may indicate active inflammation, vascular occlusion, ischemia, or secondary abnormal vessel growth. (PMC)
A hemorrhage does not always mean permanent damage, but it does usually mean the eye needs careful evaluation. Doctors want to know whether the bleeding reflects ongoing inflammation, vessel closure, retinal ischemia, or neovascularization. The answer affects whether treatment should emphasize stronger systemic control, retinal laser, local therapy, or a combination of approaches. (PMC)
Scarring: what patients fear most in the long term
Scarring is frightening because patients understand that a scar sounds permanent. In the retina, scarring can result from repeated inflammation, ischemic injury, prior hemorrhage, or healing after tissue damage. Retinal scarring does not always mean severe vision loss, because the effect depends on location. A scar away from the macula may cause few symptoms. A scar involving central retina can permanently reduce fine vision. (Mayo Clinic)
This is why doctors become more aggressive about prevention once there are signs of repeated flares or chronic leakage. The longer inflammation continues, the greater the chance of structural damage. In some patients, the treatment discussion shifts from “How do we settle this flare?” to “How do we prevent future episodes before more scarring occurs?” That often leads to maintenance therapy rather than short bursts of treatment alone. (NCBI)
Vessel blockage and ischemia: when prognosis changes more sharply
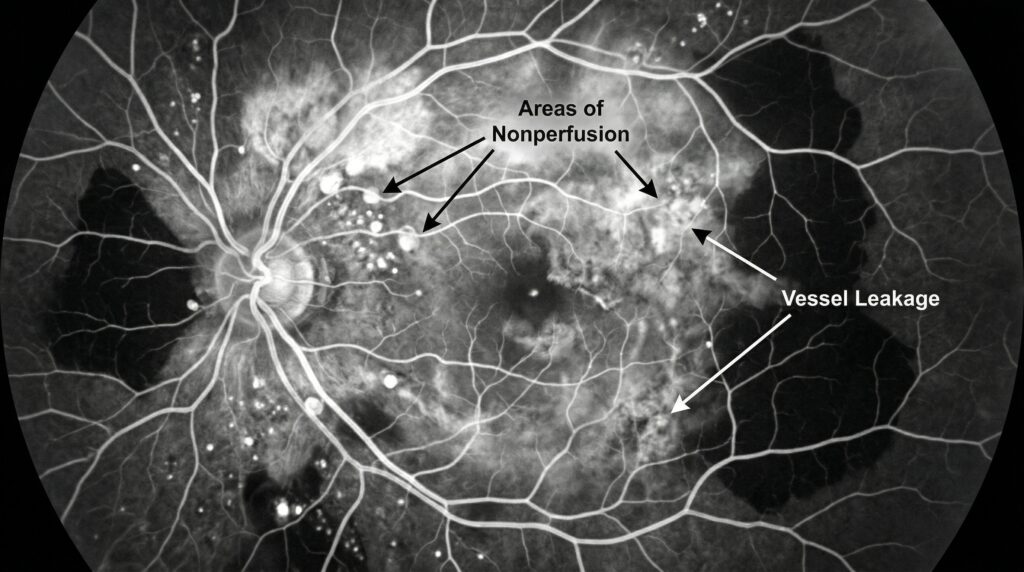
Not all retinal vasculitis behaves the same way. Some cases are mainly “leaky.” Others are “occlusive,” meaning the inflamed vessels begin to narrow or close. Occlusive retinal vasculitis is especially concerning because blocked vessels reduce blood flow to the retina. When retinal tissue is deprived of oxygen, ischemia develops. Ischemic retina can stop functioning normally and may release signals that drive abnormal new blood vessel growth. Those new vessels are fragile and can bleed. (PMC)
This is one of the clearest examples of how retinal involvement changes prognosis. A patient with mild leakage but preserved perfusion may do well with appropriate inflammation control. A patient with widespread capillary nonperfusion or neovascularization may need a more urgent and multi-layered treatment strategy, including control of inflammation plus treatment of ischemic retinal complications. (PMC)
How doctors decide the treatment path
Patients often imagine there is one standard treatment ladder for retinal vasculitis. In reality, treatment planning usually depends on five questions.
The first question is whether the cause is infectious or non-infectious. This is critical. If an infection such as tuberculosis, syphilis, toxoplasmosis, herpes viruses, or another infectious cause is driving the inflammation, suppressing the immune system without treating the infection can be harmful. On the other hand, if the vasculitis is autoimmune or idiopathic, corticosteroids and steroid-sparing immunosuppressive treatment may be central to control. (PMC)
The second question is whether the macula is involved. If OCT shows macular edema, preserving central vision becomes an urgent treatment target. The third question is whether there is retinal ischemia or vessel occlusion. The fourth is whether there is active bleeding or neovascularization. The fifth is whether this is a one-time event, a relapsing condition, or chronic disease that will likely need long-term suppression. (NCBI)
The role of imaging
Modern retinal imaging has changed how retinal vasculitis is managed. Optical coherence tomography, or OCT, is one of the most useful tools because it can show macular edema clearly and noninvasively. Fluorescein angiography remains important for identifying vessel leakage, staining, occlusion, and areas of capillary nonperfusion. Widefield imaging can be especially helpful because inflammation and ischemia may be more extensive in the retinal periphery than a standard examination suggests. Some specialists also use OCT angiography in selected cases. (PMC)
For patients, this means treatment changes are often based not just on symptoms but on what the scans show. A patient may feel “about the same,” yet the angiogram may show worsening peripheral nonperfusion. Another patient may have less visible inflammation on examination, but OCT may reveal persistent cystoid macular edema that still threatens vision. That is why scan-based follow-up is so important. (PMC)
Steroids are often the first step, but not always the last step
Corticosteroids are commonly used to control ocular inflammation quickly. Depending on the situation, they may be given as eye drops, tablets, injections around the eye, injections inside the eye, or intravenous treatment in severe disease. But retinal vasculitis often teaches us a practical lesson: fast control is not the same as long-term control. If disease keeps returning or if the steroid dose required is too high, doctors usually consider steroid-sparing immunomodulatory therapy. (NCBI)
This is another point where complications matter. A patient with mild disease and no retinal threat may be managed differently from a patient with recurrent vasculitis, macular edema, or occlusive changes. In more severe or relapsing cases, treatment may move earlier toward systemic immunosuppressive drugs or biologic agents, often in collaboration with a uveitis specialist or rheumatologist. (PMC)
When treatment needs to target both inflammation and edema
Macular edema can improve when inflammation is controlled, but not always fully or quickly. Some patients continue to have edema even as overt inflammation settles. That is one reason uveitic macular edema is considered one of the most challenging complications in ophthalmology. Persistent edema can require local corticosteroid treatment, systemic treatment adjustment, or other targeted approaches depending on the clinical setting and the patient’s overall health. (NCBI)
Patients are often surprised by this. They may assume that once the eye is “less inflamed,” the vision should immediately normalize. But swelling in the macula can take time to resolve, and chronic edema can leave lasting changes. That is why doctors sometimes continue treatment or intensify therapy even when redness or discomfort has improved. The main concern is not how the eye feels on the outside. It is whether the retina, especially the macula, is truly recovering. (American Academy of Ophthalmology)
When laser or retinal procedures enter the discussion
When retinal vasculitis causes significant ischemia, neovascularization, or recurrent hemorrhage, treatment may expand beyond anti-inflammatory medicine alone. Retinal laser photocoagulation is sometimes used to treat ischemic peripheral retina and reduce the drive for fragile abnormal blood vessel growth. In selected cases, surgical treatment may be needed for non-clearing vitreous hemorrhage or traction-related complications. (PMC)
This is exactly the sort of treatment shift that patients notice and remember. The moment the conversation changes from tablets or injections to laser or surgery, it becomes obvious that retinal complications have altered the course of care. That does not automatically mean the outlook is poor. It means the disease has moved from pure inflammation into a stage where protecting the retina may require more than one kind of treatment. (PentaVision)
What prognosis really depends on
Patients often want one simple answer about prognosis, but retinal vasculitis does not allow that. Prognosis depends on the cause, the speed of diagnosis, the degree of inflammation, whether the disease is infectious or non-infectious, the amount of retinal ischemia, the presence of macular edema, and whether damage has already become structural rather than reversible. (PMC)
In general, vision outcomes are more favorable when inflammation is treated early, when macular edema is controlled before it becomes chronic, and when occlusive disease is limited. Prognosis becomes more guarded when there is recurrent bleeding, central retinal scarring, extensive capillary nonperfusion, or repeated relapses that require ongoing high-dose steroids. (NCBI)
That said, many patients do better than they fear at the start. Even serious retinal inflammation can sometimes be stabilized effectively with modern imaging and individualized treatment. The important thing is not to underestimate the condition or delay specialist care. (PMC)
Practical advice for patients living with retinal vasculitis
One of the best things a patient can do is attend follow-up visits even when vision seems stable. Retinal vasculitis can sometimes worsen on imaging before the patient notices a dramatic new symptom. Missing reviews can allow macular edema, ischemia, or recurrent inflammation to progress quietly. (PMC)
Patients should also understand the treatment goal clearly. Ask your doctor whether the main concern right now is active vessel inflammation, macular edema, ischemia, bleeding, or prevention of relapse. Those are different clinical targets, and knowing which one is driving your plan makes treatment easier to understand. This is especially helpful when several medicines are being used for different reasons. (PMC)
It is also important to report changes such as new blur, distortion, floaters, reduced side vision, flashes, or a curtain-like shadow promptly. These symptoms can signal worsening macular edema, vitreous hemorrhage, retinal tears, or other complications that need urgent assessment. (Mayo Clinic)
If your doctors are investigating for an underlying cause, that part of the workup matters. Retinal vasculitis may be connected to a body-wide inflammatory or infectious condition, and treatment often works best when the eye disease and the underlying trigger are addressed together. (PMC)
When to see a doctor urgently
Any patient with retinal vasculitis should seek prompt ophthalmic review for sudden vision drop, new distortion, new floaters, flashing lights, increasing blind spots, eye pain with worsening blur, or any report of new bleeding or retinal swelling on follow-up imaging. Uveitis and retinal inflammation can lead to long-term vision loss if treatment is delayed. (Mayo Clinic)
Final thoughts
When patients mention retinal vasculitis together with scarring, hemorrhages, and macular edema, they are focusing on exactly the right issues. These are not minor side notes. They are the findings that most often change the conversation from routine inflammation control to vision-preserving strategy.
The main lesson is simple. Once the retina, especially the macula, is involved, doctors start thinking in layers. They must identify the cause, control inflammation, protect central vision, watch for vessel closure, treat ischemic complications, and prevent recurrence. In that sense, retinal involvement does change prognosis and treatment—but it also gives doctors a clearer roadmap for what needs attention first.
If you have been diagnosed with retinal vasculitis or inflammatory macular edema, do not judge progress only by how your eye feels day to day. The important story is often in the scans, the blood vessel status, and whether the macula is recovering. Early specialist care and regular monitoring can make a major difference.
Book an appointment with our ophthalmologist or uveitis specialist for a detailed retinal evaluation if you have been told you have retinal vasculitis, macular edema, retinal bleeding, or inflammatory changes at the back of the eye.
References
- American Academy of Ophthalmology, “What Is Macular Edema?” (American Academy of Ophthalmology)
- Agarwal A, et al. “A Comprehensive Update on Retinal Vasculitis.” PMC / PubMed. (PMC)
- NCBI Bookshelf, “Uveitic Macular Edema.” (NCBI)
- Mayo Clinic, “Uveitis: Symptoms and causes” and “Uveitis: Diagnosis and treatment.” (Mayo Clinic)
- Retinal Physician, “Diagnosis and Management of Retinal Vasculitis.” (PentaVision)





