
A first episode of uveitis often feels frightening because it affects vision suddenly and the word itself is unfamiliar. Many people worry they are going blind. Uveitis can be serious, but prompt treatment is meant to calm inflammation quickly and protect sight. The first few weeks usually involve frequent drops or other medicines, close follow-up, and gradual improvement rather than an overnight fix. Recovery time depends on which part of the eye is inflamed and how severe it is, but many first-time cases, especially anterior uveitis, improve over days to weeks with proper care.
Why First-Time Uveitis Feels So Scary—and What Usually Happens in the First Few Weeks
If you have just been told that you have uveitis, you are not overreacting if you feel scared. Most patients do.
The fear comes from a few very human thoughts that appear almost immediately. “Why is my vision blurry?” “Is this permanent?” “Could I go blind?” “How long will this take to settle?” On top of that, the eye may be painful, light-sensitive, red, or full of floaters. Many people have never even heard the word uveitis before the day they are diagnosed. That makes the whole experience feel more alarming. (nhs.uk)
As an ophthalmologist, I often tell patients that two things can be true at the same time. First, uveitis is not something to ignore. It can threaten vision if it is severe, affects the back of the eye, or is left untreated. Second, a first episode does not automatically mean permanent damage, lifelong medication, or blindness. Early treatment is specifically designed to control inflammation, ease symptoms, and reduce the chance of complications. (Mayo Clinic)
That balance is important. We should take uveitis seriously, but we should not assume the worst.
What uveitis actually is
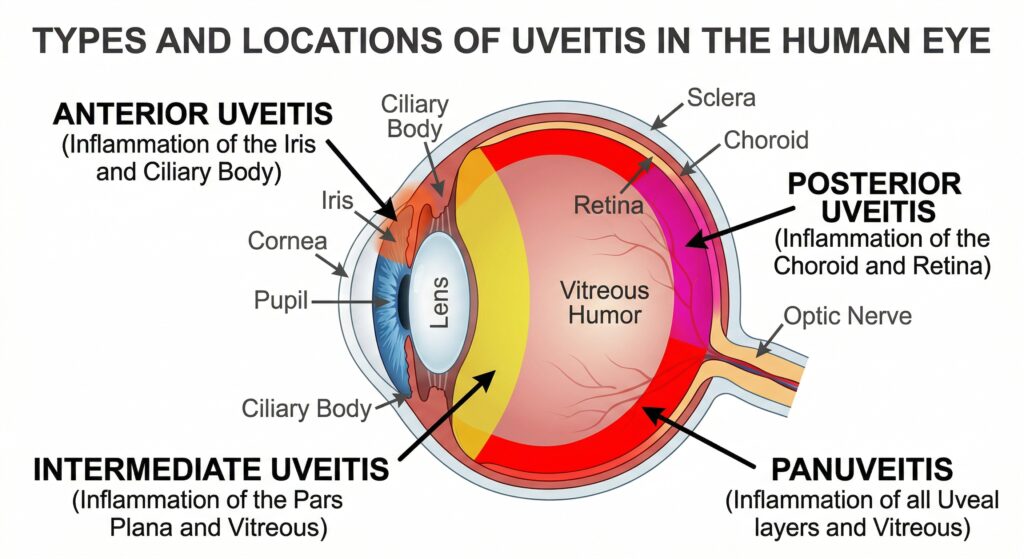
Uveitis means inflammation inside the eye. The term comes from the uvea, which includes structures such as the iris in the front of the eye, but doctors use “uveitis” more broadly for inflammation affecting several internal eye tissues. Different forms are named by location: anterior uveitis in the front, intermediate uveitis more centrally, posterior uveitis in the back, and panuveitis when several areas are involved. The type matters because symptoms, treatment, and recovery can differ quite a lot. (National Eye Institute)
For first-time patients, the most common form is anterior uveitis, also called iritis. This tends to affect the front of the eye and often causes redness, aching, sensitivity to light, and blurred vision. It usually starts suddenly. That sudden start is one reason it feels so frightening. A patient can feel fine on Monday and by Tuesday be unable to tolerate light or read comfortably. (EyeWiki)
Posterior or panuveitis can feel different. Instead of a red painful eye, the main symptoms may be floaters, hazy vision, patchy missing vision, or a general sense that sight is “off.” These forms often heal more slowly than inflammation limited to the front of the eye. (National Eye Institute)
Why the diagnosis triggers so much fear
There is a psychological side to first-time uveitis that doctors should not overlook.
Vision symptoms create immediate anxiety because eyesight feels deeply tied to independence. When a person suddenly cannot see clearly, even for a short time, the mind naturally jumps ahead to worst-case scenarios. The internet adds to this fear. Patients often find forum posts from people with severe or recurrent disease. Those stories are real, but they do not represent every first episode. Mild and moderate cases that improve with treatment are simply less likely to generate dramatic posts online. That is why early medical advice can feel very different from what frightened internet searching suggests.
Another reason for fear is uncertainty. A broken bone has a rough timeline. A cold has a rough timeline. Uveitis does not always behave that neatly. The speed of recovery depends on the cause, the location of inflammation, the severity at presentation, and whether complications such as raised eye pressure or macular edema are present. Mayo Clinic notes that recovery depends partly on the type of uveitis, and that disease affecting the back of the eye tends to heal more slowly than disease in the front. (Mayo Clinic)
This is why patients may hear phrases like “we need to monitor how you respond” or “we will taper treatment based on the inflammation.” That uncertainty is medically normal, but emotionally it can be hard.
What causes uveitis, and why doctors sometimes cannot give one simple answer
Many patients expect one clear cause. Sometimes we can identify one. Sometimes we cannot.
Uveitis can be linked to autoimmune or inflammatory diseases, infections, eye injury, and, more rarely, other conditions. NHS lists autoimmune conditions, infections such as herpes viruses and toxoplasmosis, eye injury, and rarely eye growths among the possible causes. National Eye Institute explains that inflammation may happen when the immune system is fighting an infection, or when the immune system attacks healthy tissue in the eye. (nhs.uk)
But in many first-time cases, especially anterior uveitis, no definite cause is found right away. That can be frustrating, but it is common. “We do not yet know the exact trigger” does not mean the diagnosis is uncertain or that the treatment plan is weak. It simply means the inflammation is real even when the trigger is not obvious on day one. AAO educational material also notes that acute anterior uveitis can occur as an isolated problem without a systemic association, and targeted testing is often more useful than a broad fishing expedition. (EyeWiki)
What the first few days usually feel like
The first few days are often the hardest emotionally.
If the inflammation is in the front of the eye, patients commonly notice pain, redness, light sensitivity, blur, and a small or irregular pupil. The light sensitivity can be surprisingly intense. Walking outdoors may feel unbearable. Looking at a phone screen can hurt. That discomfort does not always mean the disease is getting worse hour by hour; it is a common symptom of irritation and inflammation in the iris and nearby tissues. (nhs.uk)
Blurred vision can come from several things at once. There may be inflammatory cells in the front chamber of the eye, corneal changes from inflammation, spasm of the focusing muscle, or swelling deeper in the eye. In posterior disease, floaters and haze may be more prominent because inflammatory cells involve the vitreous or retina. (National Eye Institute)
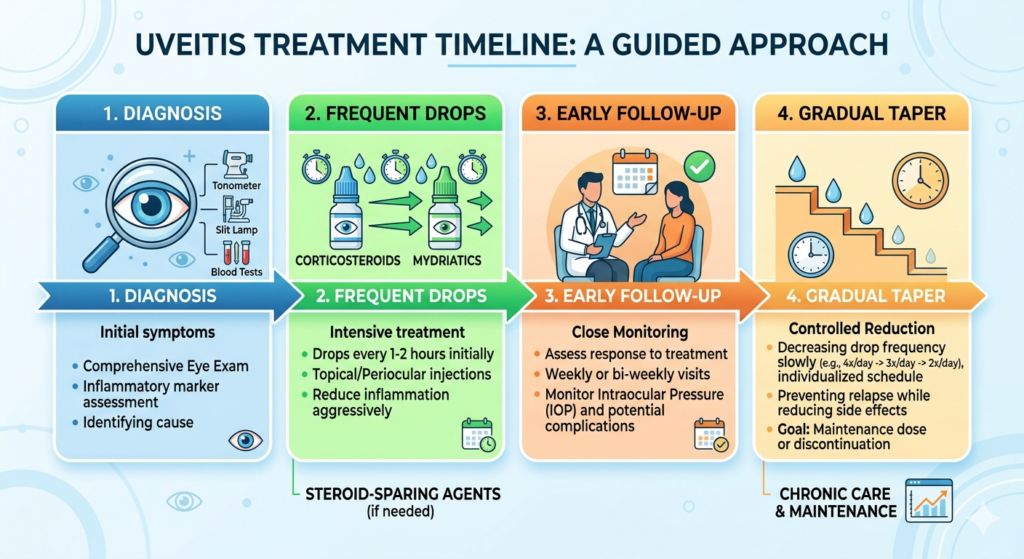
Many patients are also startled by how intensive the treatment can seem at first. For anterior uveitis, steroid eye drops may be prescribed very frequently in the beginning, then reduced gradually over several weeks. A separate drop may be used to widen the pupil. This helps relieve pain from iris spasm and can reduce the risk of the iris sticking abnormally to the lens. AAO, NHS, and NHS hospital guidance all describe this early pattern of treatment. (American Academy of Ophthalmology)
That does not mean your eye is “failing treatment.” It means early, aggressive control of inflammation is often the correct approach.
Why the drops can feel strange
Patients often worry that the treatment itself is making things worse because the drops can make vision temporarily more blurry or make the pupil stay large.
This is common. Steroid drops do not usually create a dramatic immediate feeling of relief the way a painkiller might. They work by reducing inflammation over time. Dilating drops can cause near vision blur and light sensitivity because the pupil is wider and focusing is reduced. That can make reading and screen work difficult for a few days, sometimes longer. These effects are often part of treatment rather than a sign of damage. (American Academy of Ophthalmology)
A very common patient experience is this: “The pain is a bit better, but my vision is still blurry, so I’m scared it isn’t working.” In real life, symptoms do not always improve together. Pain and light sensitivity may ease before vision fully clears. That can still represent progress.
What usually happens in the first week
In the first week, the most important goals are to confirm the diagnosis, rule out dangerous mimics, begin the right treatment, and monitor the eye closely.
Your ophthalmologist may check visual acuity, eye pressure, the cornea, the anterior chamber, the retina, and whether there are signs suggesting infection or an associated systemic condition. Depending on the pattern of inflammation and your symptoms, blood tests or imaging may be ordered, but not everyone needs a huge laboratory workup immediately. Modern uveitis care favors focused testing guided by the clinical picture. (EyeWiki)
For many patients with uncomplicated anterior uveitis, the first week is when pain begins to ease and the eye starts looking less angry. Vision may begin to improve, but it may still fluctuate. People often notice that mornings are better than evenings, or that the eye feels worse under bright lights or after long screen use. These ups and downs are common and do not automatically mean treatment failure.
If the inflammation is moderate to severe, or if it is not just in the front of the eye, treatment may involve tablets, injections around the eye, or medicines aimed at a specific infection or immune process. Mayo Clinic and NEI both note that some patients need treatment for months to years depending on the type and cause of uveitis. That sounds intimidating, but it applies more often to recurrent, chronic, intermediate, posterior, or panuveitis than to a single mild first episode of anterior disease. (Mayo Clinic)
What usually happens in weeks two to four
This is the stage where many patients begin asking the most common question: “Will my vision come back?”
The honest answer is that many patients do improve, but the speed is variable. In anterior uveitis, improvement often happens over days to weeks. AAO notes that anterior uveitis can start suddenly and symptoms can last many weeks. Hospital patient leaflets similarly describe frequent drops at first, then a gradual reduction over several weeks. (American Academy of Ophthalmology)
That phrase “many weeks” matters. It tells us that a person can still be in a normal recovery window even if they are not back to perfect vision after a few days. Patients often expect the eye to recover like an infection cleared by an antibiotic in 48 hours. Uveitis usually does not behave that way.
In this period, several paths are possible:
A patient may improve steadily, need fewer drops, and recover well.
A patient may feel better but still have mild blur due to residual inflammation, medication effects, or a complication such as macular edema.
A patient may improve, then flare slightly during tapering, requiring the treatment plan to be adjusted.
A patient with disease in the back of the eye may improve more slowly and need imaging and longer follow-up. (Mayo Clinic)
This is why follow-up appointments are so important. In uveitis, how the eye looks under examination often guides treatment better than symptoms alone.
Why vision may not snap back immediately
There are a few common reasons vision may lag behind symptom improvement.
One is simple inflammation. Even when the eye is moving in the right direction, the tissues need time to settle.
Another is the effect of dilating drops, which can blur near vision and increase light sensitivity.
A third reason is swelling in the central retina, called macular edema, which can blur or distort vision. The American Academy of Ophthalmology describes macular edema as fluid buildup in the macula that can make vision blurry and colors washed out. In uveitis, this can be one of the reasons vision is slower to recover and one of the complications doctors monitor carefully. (American Academy of Ophthalmology)
Raised eye pressure is another issue your doctor may check for, because both inflammation and steroid treatment can affect pressure. Long-term steroid use can also increase the risk of cataract and glaucoma, which is why doctors try to control inflammation while avoiding unnecessary prolonged high-dose steroid exposure. (National Eye Institute)
None of this means a bad outcome is inevitable. It means the first few weeks are a period of careful watchfulness.
When fear of blindness is understandable—and when it needs perspective
Uveitis can cause permanent vision loss if inflammation is severe, recurrent, chronic, infectious, untreated, or complicated. That is why urgent evaluation matters. NHS advises urgent assessment for eye pain, light sensitivity, or vision change, and emergency care for loss of vision. Mayo Clinic also stresses that early diagnosis and treatment are important to prevent complications and save vision. (nhs.uk)
At the same time, the presence of fear does not tell us the eventual outcome. Many eyes with vision affected by uveitis do improve. One large PubMed-indexed study of visually impaired uveitic eyes found that the estimated six-month incidence of gaining at least two lines of visual acuity was 52%, though that research involved a broad range of cases and complications, not just straightforward first-time anterior uveitis. So it should be read as supportive, not as a personal prediction. (pubmed.ncbi.nlm.nih.gov)
In everyday clinical practice, what matters most early on is not whether you can predict the whole future on day one. It is whether the inflammation is being recognized, treated, and followed appropriately.
Practical tips for getting through the early weeks
The first is to take the drops exactly as prescribed. With uveitis, timing matters. Too little treatment can let inflammation continue. Stopping suddenly without guidance can lead to rebound inflammation.
The second is to attend follow-up even if the eye feels better. Uveitis can look quieter or more active on examination than symptoms alone would suggest.
The third is to protect yourself from light if you are sensitive. Sunglasses outdoors and reduced screen brightness can help you function while the eye settles.
The fourth is not to compare your recovery too closely with someone else’s forum story. Uveitis is a category, not a single disease with one timetable.
The fifth is to tell your doctor about new symptoms outside the eye, such as joint pain, skin changes, ulcers, bowel symptoms, recent infections, or shingles history, because these details can help identify an underlying cause. (nhs.uk)
When to seek urgent help again
You should contact your eye doctor urgently or seek urgent care if pain is worsening, vision drops suddenly, you develop a curtain-like shadow, severe redness worsens, you cannot tolerate light at all, or new symptoms appear after an apparent improvement. Complete or near-complete vision loss should be treated as an emergency. (nhs.uk)
Also call promptly if treatment side effects are becoming difficult, or if you are unsure whether you used the drops correctly. In eye inflammation, it is better to ask early than to guess.
The message I most want first-time patients to hear
A first attack of uveitis feels scary because it is scary to have your eye suddenly hurt, blur, or flood with light sensitivity. The fear is real. But fear is not the same as fate.
Most patients need reassurance that recovery is usually a process, not a single dramatic moment. The eye may improve in stages. The diagnosis may take more than one visit to fully classify. The drops may be frequent at first and then slowly tapered. Vision may return gradually rather than all at once. And yes, many first-time patients do ask the exact same question you are asking now: “Will I see normally again?” That is a very normal question, and one your ophthalmologist expects. (American Academy of Ophthalmology)
What matters most in the first few weeks is prompt treatment, good follow-up, and not losing heart if the improvement is uneven. In many cases, especially anterior uveitis, the story in the first few weeks is not one of steady decline. It is one of careful treatment, close observation, and gradual recovery. (National Eye Institute)
If you have been newly diagnosed with uveitis, book and keep your follow-up appointments with your ophthalmologist, use your medication exactly as instructed, and report any sudden worsening right away. Early care gives us the best chance to protect your vision.

References
- American Academy of Ophthalmology. What Is Uveitis? https://www.aao.org/eye-health/diseases/what-is-uveitis
- National Eye Institute (NIH). Uveitis. https://www.nei.nih.gov/eye-health-information/eye-conditions-and-diseases/uveitis
- NHS. Uveitis. https://www.nhs.uk/conditions/uveitis/
- Mayo Clinic. Uveitis: Symptoms and causes. https://www.mayoclinic.org/diseases-conditions/uveitis/symptoms-causes/syc-20378734
- Mayo Clinic. Uveitis: Diagnosis and treatment. https://www.mayoclinic.org/diseases-conditions/uveitis/diagnosis-treatment/drc-20378739





