
Orbital decompression for thyroid eye disease is not only about appearance. In the right patient, it can protect vision, help the eyelids close better, and reduce bulging and pressure. The best oculoplastic team in India is usually the one with focused orbit-oculoplasty training, real TED experience, proper CT-based planning, clear discussion of risks, and coordinated care with endocrinology and, when needed, ENT or strabismus specialists. A good team should also tell you whether your disease is still active or whether it is the right time for surgery. (American Academy of Ophthalmology)
Need Orbital Decompression for Thyroid Eye Disease? How to Choose the Right Oculoplastic Team in India
If you or a family member has already been told that orbital decompression may be needed, you are no longer searching for basic information. You are trying to answer a much harder question: where should I go, and whom should I trust?
That is a very reasonable question. Thyroid eye disease, also called Graves’ eye disease or TED, can cause bulging of the eyes, irritation, light sensitivity, pressure, double vision, and in severe cases, loss of vision. Orbital decompression is the surgery used to create more room in the eye socket so the eye can move back and the crowded tissues around the optic nerve have more space. In the right setting, this is a sight-saving operation. In other patients, it is part of later rehabilitation to improve bulging, exposure, and comfort after the disease has settled. (American Academy of Ophthalmology)
This is exactly why choosing the surgeon is not just about finding “the best eye doctor.” Orbital decompression for TED sits at the intersection of orbit surgery, thyroid disease, imaging, strabismus, eyelid position, and sometimes sinus surgery. A team that does this regularly tends to think differently from a team that only does it occasionally. The difference often shows up in planning, timing, risk counseling, and follow-up.
First, understand what orbital decompression actually does
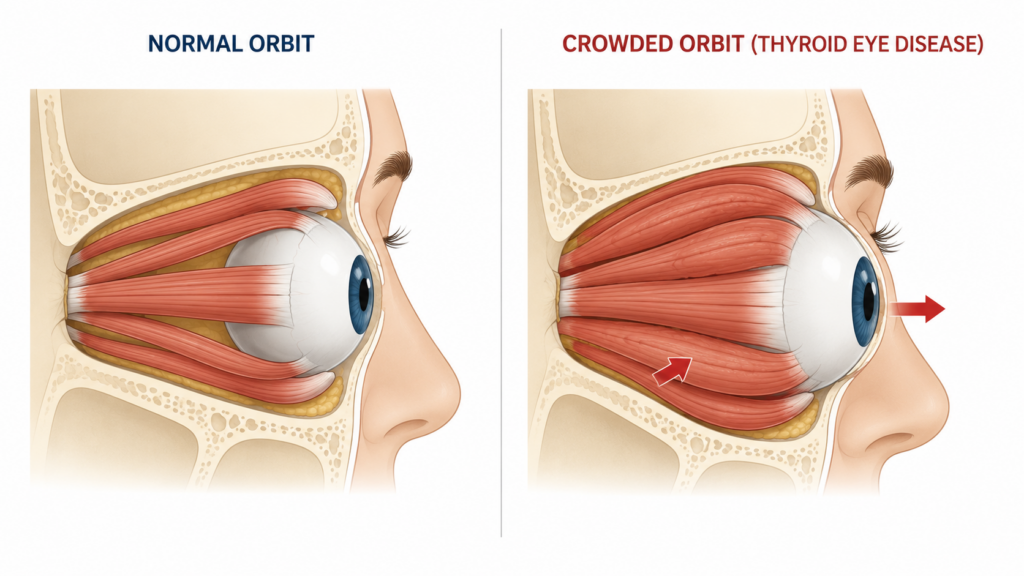
The eye sits inside a bony socket called the orbit. In thyroid eye disease, the immune system attacks tissues around the eye, especially the eye muscles and orbital fat. Those tissues enlarge, but the bony socket does not. The result is crowding. That crowding can push the eye forward, keep the lids from closing well, dry the surface of the eye, and in severe cases compress the optic nerve. (NIDDK)
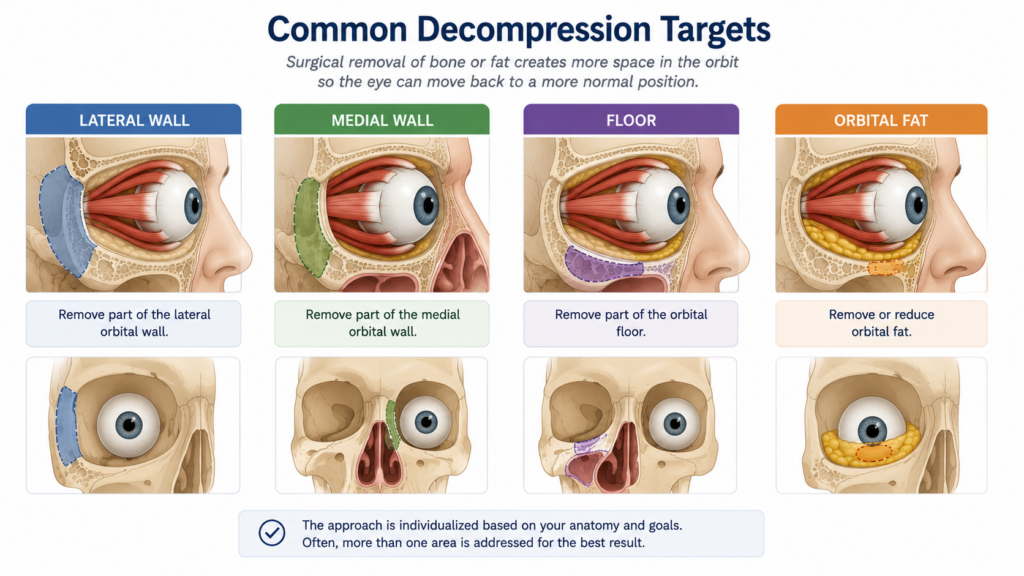
Orbital decompression works by increasing the available space. Depending on the patient’s anatomy and goal, the surgeon may remove part of the lateral wall, the medial wall, part of the floor, orbital fat, or a balanced combination of these. This is why there is no single “standard decompression” that suits everyone. A patient whose main problem is optic nerve crowding may need a different approach from someone whose main complaint is severe bulging or poor eyelid closure. (Imperial College Healthcare)
When is decompression really needed?
Patients are often told about decompression at two very different stages of TED, and this can cause confusion.
The first is urgent or sight-saving decompression. International guidance says that sight-threatening Graves’ orbitopathy is treated urgently, usually with high-dose intravenous steroids first, and if the response is poor or absent, orbital decompression is performed promptly. This is the situation when the optic nerve is threatened or the cornea is at serious risk because the eye is too exposed. (PubMed)
The second is rehabilitative decompression. This is more common in patients who are no longer in the hot, inflamed phase of disease but are left with residual bulging, eyelid closure problems, chronic exposure, facial asymmetry, or pressure that affects comfort and confidence. The 2021 EUGOGO guideline states that rehabilitative surgery, including orbital decompression, is indicated for inactive residual disease. (PubMed)
This is one of the most important questions to ask your doctor: Is my disease active and inflamed, or inactive and stable? A good team should answer that clearly. If the disease is still active, surgery may still be needed in urgent cases, but many patients are first managed with lubrication, thyroid control, smoking cessation, and medical treatment directed at inflammation. Smoking is especially important because Mayo Clinic notes that smoking worsens thyroid eye disease. (Mayo Clinic)
Why the right team matters more than a single famous name
A strong TED service is not just one skilled pair of hands. It is a system.
Mayo Clinic describes thyroid eye disease as a condition that requires multispecialty evaluation, with involvement of endocrinologists, ophthalmologists, and ENT surgeons for optimal management. That matches what many experienced orbit units already know: the best outcomes usually come from coordinated care, not siloed care. (Mayo Clinic)
For example, if your main issue is bulging, decompression may be the first operation. But if you also have double vision or eyelid retraction, the order of surgery matters. Current reviews and consensus guidance generally place orbital decompression first, followed by strabismus surgery if needed, and then eyelid surgery, because decompression can change eye position and eyelid relationships. If a surgeon rushes to “fix the lids” before discussing decompression, that is often not the full TED plan. (PMC)
In practical terms, the right team should be able to answer three questions without sounding vague. First, is vision at risk? Second, what is the real goal of surgery in your case: save vision, reduce bulging, improve closure, or improve appearance and symmetry? Third, what other procedures might still be needed later? A surgeon who gives only a one-line answer such as “we will push the eyes back” is not giving you the whole picture.
What should you look for in an oculoplastic team in India?
India has a strong and mature oculoplasty community. The Oculoplastics Association of India, founded in 1987, describes itself as the premier professional body dedicated to ophthalmic plastic and reconstructive surgery, with members focused on the orbit, eyelids, lacrimal system, and related areas. The All India Ophthalmological Society also recognizes oculoplastic surgery as a formal subspecialty within its FAICO system. In other words, there is a real subspecialty pathway in India; this is not an informal interest area. (OCULOPLASTICS ASSOCIATION OF INDIA)
That means it is fair for you to ask direct questions about training. Did the Occuloplasty surgeon complete formal orbit-oculoplasty fellowship training? Does the surgeon’s routine practice include orbital surgery and thyroid eye disease, or mostly general ophthalmology with occasional orbit cases? Large Indian eye institutes also run dedicated orbit and oculoplasty fellowships, which reflects the depth of the field and the fact that this surgery is best learned through structured training and volume.
Please remember, a degree or association membership alone does not prove surgical judgment. But it does tell you that you are dealing with a surgeon who works inside the correct subspecialty ecosystem. For a surgery as nuanced as decompression, that matters.
The signs of a team you can trust
A trustworthy team usually does several things well before talking about the operation date.
They document the problem carefully. That means listening to your symptoms, measuring proptosis, checking vision, checking the ocular surface, asking about diplopia, and obtaining imaging when needed. Consensus guidance identifies noncontrast CT as the standard imaging modality because it is widely available and helps assess the orbit for decompression surgery. Preoperative high-resolution CT or MRI is also emphasized in surgical reviews of orbital decompression. (PMC)
They explain the why behind the chosen technique. Some patients need fat decompression. Some need lateral wall work. Some need a balanced decompression. Some may benefit from an endoscopic medial wall approach with ENT collaboration. There is no prize for the most aggressive surgery; the right surgery is the one that matches the anatomy and the goal. (Imperial College Healthcare)
They speak honestly about risk. Imperial College Healthcare’s patient information notes that decompression can involve soreness, lid swelling, temporary cheek or dental numbness, worsening or new double vision, damage to tear drainage in some medial wall cases, and a very rare risk to sight. Mayo Clinic also notes double vision as a possible complication. No good surgeon should minimize these issues, because risk counseling is not pessimism. It is professionalism.
They tell you what comes after surgery, not just what happens during surgery. Patients often focus on the theatre day, but TED care is rarely finished there. A good team prepares you for follow-up, swelling, surface care, and the possibility that muscle or lid surgery may still be needed later.
Questions you should ask before choosing a surgeon
When I advise patients, I tell them not to be shy. High-intent patients should ask high-quality questions.
Ask whether your disease is active or inactive. This affects timing and expectations. A good answer should not be vague. The team should explain whether the goal is urgent vision protection or later rehabilitation. (PubMed)
Ask what part of the orbit they plan to decompress and why. You do not need to master the anatomy, but you do deserve a simple explanation.
Ask how often they operate on TED specifically. “Orbit surgery” is a broad label. Thyroid eye disease is its own problem, with its own planning and complications.
Ask whether the center has endocrinology support and, when appropriate, ENT and strabismus support. Mayo’s model highlights exactly this kind of combined care. (Mayo Clinic)
Ask what risks are most relevant in your case. Is double vision already present? Is the aim to reduce pressure on the optic nerve? Is one eye worse? Are both eyes being done together or staged?
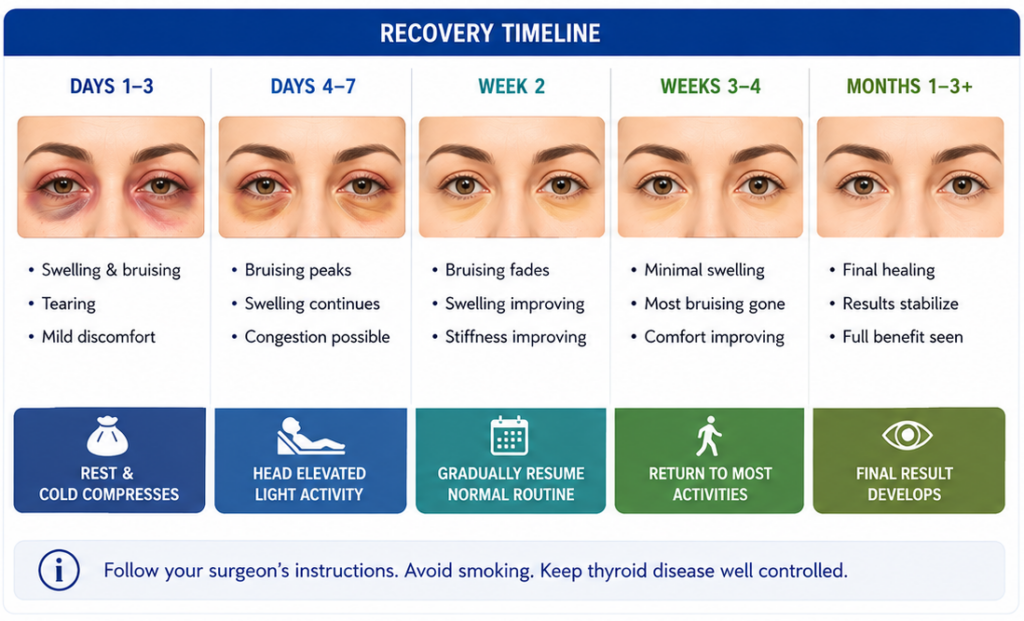
Ask what the recovery plan is. For example, patient leaflets note that after medial wall decompression, nose blowing should be avoided for a period of time, and swelling and bruising are expected for weeks. You want a team that gives precise aftercare instructions, not one that says only “come back if there is a problem.” (Imperial College Healthcare)
Ask what success means in your case. Sometimes success means saving vision. Sometimes it means reducing bulging enough for the lids to close. Sometimes it means improving symmetry, while accepting that perfect symmetry may not be realistic.
How to compare centers in India without getting lost in marketing
Patients often compare hospitals by city, social media presence, or a single famous name. That is understandable, but it is not the best filter.
A better filter is this: which center seems built for TED? Does the surgeon clearly work in orbit and oculoplasty? Does the center have CT imaging access, anesthesia support, endocrinology input, and referral pathways for strabismus or ENT if needed? Does the consultation feel thoughtful, or rushed? Do they show you how they decide timing? Do they explain why one approach is being chosen over another? These are stronger signs of quality than polished advertising.
In India, another practical issue matters: follow-up. Decompression is not a “fly in, operate, disappear” surgery. Especially if you live in another state, think about where you can realistically return if you develop swelling, worsening diplopia, sinus symptoms, or surface problems. The best center on paper is not always the best center for you if follow-up is nearly impossible. That is a judgment call, but it is an important one.
I also encourage patients to be cautious of two extremes. One is the team that pushes surgery before properly staging the disease. The other is the team that keeps delaying appropriate surgery even when bulging, exposure, or optic nerve risk is clearly affecting quality of life or sight. Good care lives in the middle: careful, timely, and individualized. (PubMed)
What to expect before and after surgery
Most decompressions are performed under general anesthesia. Patient guidance from Imperial College Healthcare notes that many patients stay one night in hospital, though this can vary by center and surgical extent. The operation itself may involve one or more orbital walls, with or without fat removal. (Imperial College Healthcare)
After surgery, swelling and tenderness are common. Some patients notice numbness over the cheek or teeth that gradually improves. Double vision can worsen or appear after decompression, which is one reason preoperative counseling matters so much. If the surgery involves the medial wall, teams usually give instructions about avoiding nose blowing and sometimes flying for a period during healing.
Recovery is not only physical. Many TED patients have already spent months or years feeling frightened by the change in their face, worried about their sight, and frustrated by incomplete answers. A good oculoplastic team understands that decompression is not “cosmetic reassurance.” It is functional, reconstructive, and often emotionally important.
When should you seek urgent care?
Do not wait for your next routine appointment if your vision drops suddenly, if the eye becomes increasingly exposed and painful, or if symptoms are rapidly worsening. Severe TED can threaten sight, and urgent evaluation is appropriate when vision is at risk. Both Mayo Clinic and NHS guidance emphasize urgent attention for vision loss related to thyroid eye disease. (Mayo Clinic)
The bottom line
If you are searching for orbital decompression in India, do not focus only on “who is the most famous surgeon.” Focus on whether the team thinks like a true thyroid-eye team.
The right oculoplastic service will assess disease activity, explain why surgery is or is not needed now, review imaging properly, talk honestly about diplopia and other risks, and coordinate care with endocrinology and other specialists when required. It will also tell you where decompression fits into the larger TED journey, because for many patients it is one stage in a carefully planned sequence, not the whole story. (Mayo Clinic)
If you are considering surgery, book a consultation with a dedicated oculoplastic-orbit specialist and bring your thyroid history, eye records, scans, and a list of questions. The best decision is usually the one made with clear anatomy, clear timing, and a team that treats TED regularly.
References
American Academy of Ophthalmology: “What Is Thyroid Eye Disease (TED) or Graves’ eye disease?” (American Academy of Ophthalmology)
Mayo Clinic: “Graves’ disease — Diagnosis and treatment.” (Mayo Clinic)
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): “Graves’ Disease.” (NIDDK)
PubMed: “The 2021 EUGOGO clinical practice guidelines for the medical management of Graves’ orbitopathy.” (PubMed)Oculoplastics Association of India (OPAI): official society overview. (OCULOPLASTICS ASSOCIATION OF INDIA)






{kind=link}