
If your eyes keep watering, the problem is not always “too many tears.” Very often, it is either dry eye causing reflex tearing or a blockage in the tear drainage pathway. Dry eye usually comes with burning, grittiness, screen discomfort, and often affects both eyes. A blocked tear duct is more likely when tears spill down one cheek, there is sticky discharge, or swelling near the inner corner of the eye. DCR surgery is usually considered when tests show a true drainage blockage, especially if watering is persistent or infections keep coming back. (Mayo Clinic)
Why Are My Eyes Watering All the Time? When Indian Patients Get Sent for DCR Surgery
One of the commonest questions I hear in clinic is this: “Doctor, my eyes water all day. Is this dryness, allergy, or a blocked tear duct?” In India, that confusion is especially common. A younger patient may spend long hours on screens, sit under a fan or air-conditioner, ride through dust and traffic, and develop dry eye that paradoxically makes the eyes water. An older patient may have a true drainage problem and need a tear-duct procedure such as DCR. Both patients complain of “watering,” but the treatment is completely different. (Mayo Clinic)
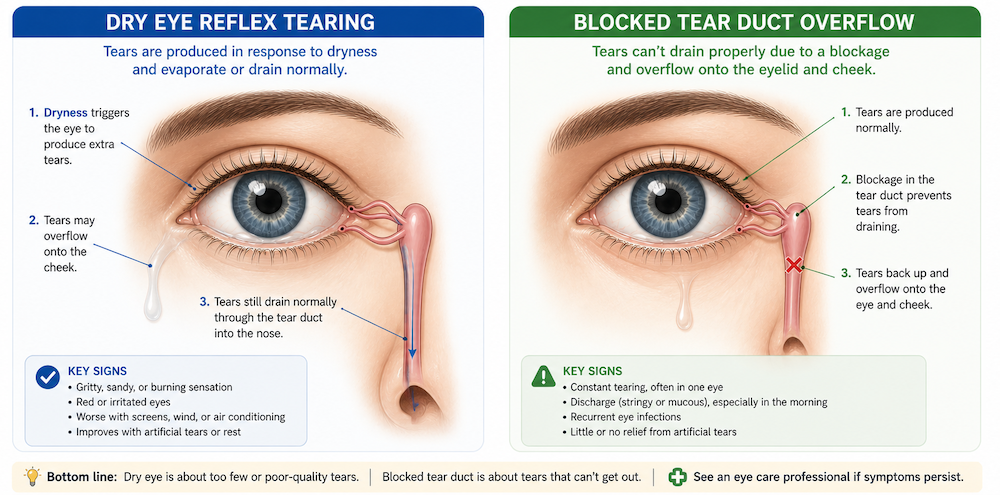
That is why persistent watering should not be reduced to a guess. Tears are being made all the time, and under normal circumstances they drain through tiny openings near the inner corner of the eyelids, pass into the tear sac, and then travel down the nasolacrimal duct into the nose. When that drainage system narrows or blocks, tears overflow onto the cheek. When the eye surface is irritated or dry, the eye may also respond by producing a flood of poor-quality reflex tears. Both situations look similar to patients, but they are not the same disease. (Guy’s and St Thomas’ NHS Trust)
Image suggestion: Simple diagram showing the tear gland, puncta, tear sac, and nasolacrimal duct into the nose.
The first big surprise: dry eyes can cause watery eyes
This sounds backwards, but it is true. Dry eye does not always mean a person has “no tears.” Many patients with dry eye have poor-quality tears, unstable tear film, or excessive evaporation. When the eye surface becomes irritated, the body tries to wash the irritation away by releasing more watery reflex tears. That is why some people say, “My eyes feel dry, burning, and gritty, but they also water constantly.” That pattern is well recognized in ophthalmology. (Mayo Clinic)
Dry eye is more likely when watering is accompanied by burning, stinging, a scratchy or sandy feeling, redness, light sensitivity, fluctuating blur, trouble with contact lenses, or symptoms that worsen during screen use. Screen-heavy routines matter because blinking often becomes incomplete or less frequent during digital work, which worsens tear evaporation. Studies from India and related digital-eye-strain literature have linked video display terminal use and screen time with dry eye symptoms. In one Indian Journal of Ophthalmology study from North India, dry eye disease prevalence was reported at 32%, with adults aged 21 to 40 affected most commonly, and video display terminal use, smoking, and contact lens use associated with dry eye. (Mayo Clinic)
This is one reason so many Indian patients in their 20s and 30s worry about a “blocked tear duct” when the real issue is ocular surface disease. The setting is familiar: long office hours, two-wheelers in wind and pollution, dry indoor air, irregular sleep, and repeated use of over-the-counter drops without a diagnosis. In that group, watering is often not a drainage problem at all. It is the eye asking for a healthier tear film. That said, dry eye is not the only answer, and persistent watering deserves a proper exam. (ijo.in)
When watering points more toward a blocked tear duct
A blocked tear duct becomes more likely when tears roll down the cheek despite the eye not feeling especially dry, when one eye is much worse than the other, when there is sticky discharge, or when the symptoms have been dragging on for months or years. Some patients notice that the watering gets worse in wind, cold weather, after a cold, or during sinus trouble. Others describe recurrent swelling or tenderness near the inner corner of the eye. (nhs.uk)
In adults, tear-duct blockage can happen because the duct narrows with age. It can also follow facial injury, nose or sinus disease, inflammation, certain medicines, or previous surgery. In the lacrimal literature, primary acquired nasolacrimal duct obstruction is commonly linked to age-related fibrosis of the duct. This is one reason I become more suspicious of a true blockage in older patients with one-sided, persistent watering and discharge. (Guy’s and St Thomas’ NHS Trust)
Sometimes blockage leads to infection of the tear sac, called dacryocystitis. That is not just a nuisance. It can present with pain, redness, swelling near the inner corner of the eye, and pus-like discharge. In chronic cases, there may simply be ongoing watering with intermittent discharge. If a patient has repeated episodes of this, DCR often enters the conversation because the underlying drainage obstruction needs to be bypassed. (NCBI)
It is not always dry eye or blocked duct
There is another important point patients should know: watering eyes are not caused only by dry eye and nasolacrimal duct blockage. Allergy, conjunctivitis, eyelid malposition such as ectropion, punctal narrowing, facial nerve weakness, some medicines, and surface irritation from a lash or foreign body can also cause watering. So if you are trying to diagnose yourself from symptoms alone, you can easily go wrong. (nhs.uk)
That is why two patients with the same complaint can walk out of clinic with completely different plans. One may get lubricant drops, blink training, lid care, and treatment for meibomian gland dysfunction. Another may be scheduled for syringing, nasal assessment, and lacrimal surgery. The complaint is the same. The cause is not. (Guy’s and St Thomas’ NHS Trust)
How ophthalmologists tell the difference
A good consultation for watering eyes should do more than hand you a bottle of drops. For dry eye, the ophthalmologist usually examines the ocular surface on a slit lamp and may assess tear-film stability and tear production using tests such as tear break-up time and Schirmer testing. For blockage, the specialist looks closely at the puncta, eyelids, and tear drainage pathway, and may flush saline through the system with a fine cannula. If DCR is being considered, examination of the inside of the nose with an endoscope may also be part of the work-up. (Guy’s and St Thomas’ NHS Trust)
This step matters more than patients often realize. Many people have mixed disease. A person can have mild dry eye plus partial drainage narrowing. Another can have watering that is mostly due to eyelid laxity or punctal stenosis, not a deep nasolacrimal block. This is why an experienced oculoplasty or lacrimal surgeon does not jump to surgery based on history alone. The anatomy has to make sense. (NCBI)
When does DCR surgery come into the picture?
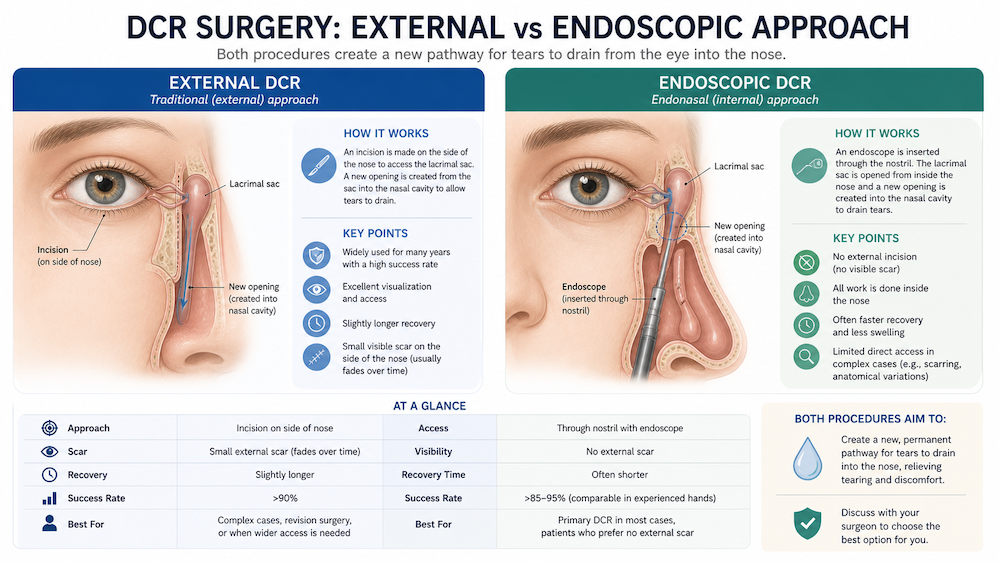
DCR stands for dacryocystorhinostomy. In simple language, it is an operation that creates a new pathway for tears to drain from the tear sac into the nose, bypassing the blocked part of the tear duct. It is not a treatment for dry eye. It is a drainage surgery for patients in whom testing shows a relevant tear-duct blockage. It is most often considered when watering is persistent and troublesome, when tears keep spilling down the face, when sticky discharge or recurrent dacryocystitis is present, or when daily life is clearly being affected. (Guy’s and St Thomas’ NHS Trust)
This is exactly where many Indian patients begin searching online for “endoscopic DCR hospital near me,” or for “DCR experiences” in cities such as Delhi, Mumbai, Bengaluru, Hyderabad, Chennai, Kolkata, Pune, or Ahmedabad. That search makes sense. But the more important question is not only which city or hospital name appears first. The real question is whether the diagnosis is correct and whether the surgeon has identified the exact level of blockage. A beautifully performed DCR will not solve watering caused mainly by dry eye. (Guy’s and St Thomas’ NHS Trust)
External DCR versus endoscopic DCR
Patients often ask whether endoscopic DCR is “better” than external DCR. The honest answer is that each has a role. In external DCR, the surgeon reaches the tear sac through a small skin incision on the side of the nose. In endoscopic or endonasal DCR, the surgeon works from inside the nose with an endoscope, so there is no skin cut and no external scar. Patient information sources from major eye units describe similar overall success rates for the two approaches, commonly around 85% to 90%. (Cambridge University Hospitals)
So how do surgeons choose? External DCR may be preferred when the smaller canaliculi near the eyelids are also blocked, while endoscopic DCR can be especially attractive when there are nasal issues such as polyps or sinus problems that may be addressed at the same sitting. Endoscopic DCR also appeals to many patients because there is no visible scar. In practice, the best option depends on the anatomy, the surgeon’s expertise, and whether nasal pathology is part of the problem. (Leeds Teaching Hospitals NHS Trust)
What patients usually want to know before surgery
When patients ask for “real experiences,” they are usually asking practical questions, not textbook definitions. Will I stay in hospital? Will there be pain? Will my eye stop watering immediately? Will there be a tube? When can I return to work?
Most DCR procedures are described as day-case surgeries, often under general anaesthesia. A temporary silicone tube or stent is commonly placed to keep the new passage open during healing. For endoscopic DCR, many patient guides describe tube removal after about 4 to 6 weeks. External DCR often also uses a stent, with removal commonly around 6 weeks, though some centres describe a longer range. (Guy’s and St Thomas’ NHS Trust)
After surgery, slight nasal bleeding, bruising, and swelling can happen. Patients are usually advised not to blow the nose for around 10 days to 2 weeks. Watering may continue for some time after the operation because swelling has to settle and the tube is still in place. That delayed improvement sometimes worries patients, but it is a known part of recovery. Many centres also advise avoiding hot drinks briefly after surgery and seeking urgent review for severe pain, marked redness, excessive discharge, or prolonged bleeding. (Guy’s and St Thomas’ NHS Trust)
The other thing patients should know is that success does not always mean “perfectly dry forever.” Some sources define success as watering stopping completely or becoming minimal, perhaps only noticeable in very windy weather. A minority of patients may need revision surgery if scar tissue closes the new opening. That is why follow-up matters almost as much as the operation itself. (Leeds Teaching Hospitals NHS Trust)
How to think about choosing a DCR centre in India
If you are searching city by city, try not to choose only on the basis of the loudest advertisement or the most dramatic online testimonial. A better filter is this: does the centre have an ophthalmologist who regularly manages lacrimal disorders, can they properly test the drainage system, do they have endoscopic evaluation when needed, and do they have a clear follow-up plan for stent care, bleeding, or infection? Because DCR work-up may include nasal endoscopy, and because endoscopic DCR may be especially useful when nasal disease coexists, a centre that can assess both the eye side and the nasal side is often preferable. That is an inference from how the procedure is evaluated and selected in specialist practice. (Guy’s and St Thomas’ NHS Trust)
In other words, the “best” DCR hospital in your city is usually the one that first proves you need DCR at all. Good lacrimal care is not about rushing every watering eye to surgery. It is about separating dry eye, eyelid problems, punctal disease, and true nasolacrimal blockage before recommending a procedure. That is the standard patients should look for, whether they are consulting in a metro city or a smaller town. (nhs.uk)
When you should seek help sooner rather than later
Please do not sit on the problem for months if the eye is watering every day and affecting work, driving, reading, or social confidence. And do not wait at all if there is pain, redness, swelling at the inner corner, sticky discharge, fever, or any change in vision. Severe eye pain or loss of vision needs urgent medical attention. Painful swelling with discharge near the inner corner raises concern for dacryocystitis, which needs prompt treatment and sometimes later definitive drainage surgery. (nhs.uk)
If the symptoms are milder and you are still sorting out the cause, lubricant drops may help when dry eye is part of the problem, and warm compresses can sometimes ease irritation. But self-treatment should not drag on indefinitely if the watering is persistent. Repeated use of the wrong drop can delay the real diagnosis. (Mayo Clinic)
The bottom line
A watering eye is a symptom, not a diagnosis. In Indian practice, the two big possibilities patients commonly hear about are dry eye and blocked tear duct, and both are real. Dry eye often causes reflex watering, especially in younger screen users. A blocked tear duct becomes more likely when watering is persistent, often one-sided, associated with discharge, or complicated by swelling and infection near the inner corner. DCR is usually recommended only when tests show that the drainage pathway is truly blocked and symptoms are significant. (Mayo Clinic)
So before you search endlessly for “best endoscopic DCR by city,” make sure the first question has been answered correctly: why is your eye watering in the first place? That single step often saves patients from months of confusion and, sometimes, from the wrong treatment altogether. (Guy’s and St Thomas’ NHS Trust)
Book an appointment with our ophthalmologist or lacrimal specialist if your eyes have been watering for more than a few weeks, if one eye is much worse than the other, or if you have discharge, swelling, or repeated infections near the inner corner of the eye.
References
- Mayo Clinic, “Dry eyes: Symptoms & causes.” (Mayo Clinic)
- NHS, “Watering eyes.” (nhs.uk)
- Guy’s and St Thomas’ NHS Foundation Trust, “Dacryocystorhinostomy surgery for blocked tear ducts.” (Guy’s and St Thomas’ NHS Trust)
- Cambridge University Hospitals, “Dacryocystorhinostomy (DCR).” (Cambridge University Hospitals)
- Indian Journal of Ophthalmology, “Prevalence and risk factors of dry eye disease in North India.” (ijo.in)





