
Blurred vision after starting steroid drops for uveitis does not always mean the treatment is failing. Very often, vision stays foggy for a while because inflammation takes longer to clear than redness and pain, because protein and inflammatory cells are still floating inside the eye, or because the dilating drops used with steroids temporarily blur focus. But persistent or worsening blur can also signal ongoing active uveitis, raised eye pressure, corneal swelling, or complications such as cystoid macular edema. The safest rule is this: improving comfort is good, but vision must still be monitored closely by your ophthalmologist.
Blurry Vision After Starting Steroid Drops: Healing, Side Effect, or a Sign Your Uveitis Is Still Active?
When patients start treatment for uveitis, they often expect a simple sequence. The eye is red and painful. Steroid drops are started. A few days later, everything should be back to normal. Real life is often less tidy than that.
One of the most common questions in clinic is this: “My redness and pain are better, but my vision is still foggy. Is that normal?” It is a very reasonable question, and it deserves a careful answer.
In many cases, blurry vision early in treatment does not mean disaster. It may simply mean that the eye is healing more slowly than the symptoms on the surface suggest. Uveitis is inflammation inside the eye. Redness and pain often improve first, while visual clarity can take longer to recover. At the same time, some of the drops used during treatment can blur vision on their own. But there are also times when persistent blur is a warning sign that inflammation is still active or that a complication is developing. (Mayo Clinic)
That is why blurred vision during uveitis treatment should never be judged by a single symptom alone. We look at the whole picture: how the eye feels, what the vision is doing, what the pressure is, whether there are inflammatory cells still present, and whether the retina or cornea has become involved. (Mayo Clinic)
Why vision can stay foggy even when the eye feels better
The most important thing to understand is that pain relief and visual recovery do not always happen at the same speed.
In anterior uveitis, which affects the front part of the eye, steroid drops reduce inflammation. As the inflammation settles, the eye often becomes less red, less light-sensitive, and less uncomfortable. That is encouraging. But inside the eye, inflammatory cells and protein can still remain in the fluid behind the cornea for some time. Patients sometimes describe this as looking through smoke, mist, or dirty glass. Even when the eye is clearly improving, the view may not yet be fully clear. (NCBI)
Another reason is that the eye’s tissues may still be recovering from the inflammatory episode itself. The iris, cornea, and lens can all be affected directly or indirectly. Even after the “fire” of inflammation starts to calm, the visual system may not reset immediately. This is one reason ophthalmologists rely on slit-lamp examination and follow-up visits rather than symptoms alone. (Mayo Clinic)
The most common harmless explanation: your dilating drops
Many patients with anterior uveitis are prescribed not only steroid drops, but also dilating drops. These are very important. They reduce pain from spasm inside the eye and help prevent the iris from sticking to the lens, which can lead to complications. But they often blur vision, especially for reading and near work, and they can also make the eye more light-sensitive. (Oxford University Hospitals)
This is probably the single most common reason patients feel confused. They assume the steroid is not working because the vision is still blurry, when in fact the prescribed dilating drop is doing exactly what it is supposed to do. If your pupil is kept large, your eye cannot focus normally, and near vision often becomes noticeably worse until the drop is reduced or stopped. (American Academy of Ophthalmology)
So yes, sometimes blurry vision during treatment is a side effect, but not necessarily a dangerous one. It may simply be the expected result of the mydriatic or cycloplegic drop your doctor added to protect the eye. (Moorfields Eye Hospital)
Image suggestion: Patient-friendly illustration showing how dilating drops enlarge the pupil and temporarily affect focusing.
Can the steroid drop itself cause blur?
Yes, but context matters.
Some eye drops can cause temporary blur immediately after they go in. This is especially true if the medication is a suspension rather than a completely clear solution, or if the surface of the eye is a little dry or irritated. That type of blur usually lasts minutes, not days. It is inconvenient, but not usually dangerous by itself. (American Academy of Ophthalmology)
Steroid drops can also contribute to longer-term side effects, particularly if treatment is prolonged or if a patient is especially sensitive. The two complications ophthalmologists watch closely for are raised eye pressure and cataract formation. Raised pressure may not cause obvious symptoms at first, but in some people it can contribute to visual disturbance and, if unchecked, damage the optic nerve. Cataract usually develops with longer or repeated steroid exposure rather than in the first few days, but it is one of the known reasons vision can remain poor over time in patients with recurrent or chronic uveitis. (NCBI)
That said, when a patient asks about blurry vision soon after starting drops, the more common causes are still active inflammation, dilating drops, dry ocular surface, or inflammation-related complications, rather than a steroid-induced cataract appearing overnight. (NCBI)
When blur means the uveitis may still be active
This is the part that matters most.
If the pain and redness are improving but vision is not improving at all, or is getting worse, we have to consider that the inflammation may not yet be adequately controlled. Uveitis can still be active even if the eye looks calmer from the outside. Blurred vision is one of the core symptoms of uveitis and decreased vision can persist when there are still inflammatory cells, flare, corneal edema, vitreous haze, or retinal involvement. (Mayo Clinic)
This is especially important because not all uveitis is limited to the front of the eye. Steroid drops are usually very effective for anterior uveitis, but eye drops alone are often not enough for inflammation located deeper in the eye. If the intermediate, posterior, or panuveitis components are present, blurred vision may persist because the real problem is not fully reachable with topical treatment alone. (Mayo Clinic)
Another important clue is floaters. If a patient says the eye is less painful but vision is still cloudy and there are many floaters, that can suggest inflammatory activity in the vitreous or back of the eye rather than simply a focusing problem from dilating drops. (Mayo Clinic)
The retina matters: cystoid macular edema and other deeper causes
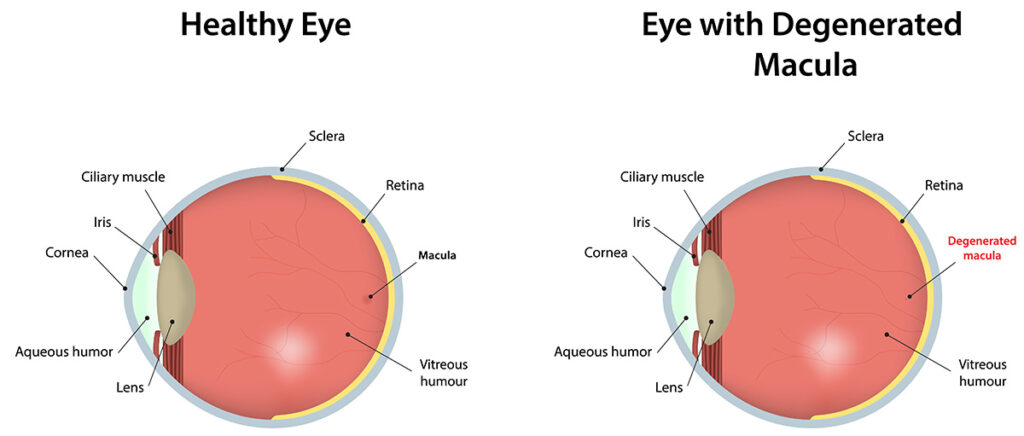
One reason vision may remain blurry despite a quieter-looking eye is cystoid macular edema, often shortened to CME. This means swelling in the macula, the part of the retina responsible for sharp central vision. Patients may describe letters as smudged, faces less crisp, or straight lines slightly distorted. Sometimes the front of the eye looks much better, yet the vision still does not recover because the retina is swollen. (NCBI)
This is one reason follow-up visits are so important. Your ophthalmologist may need to examine the retina carefully or perform imaging such as OCT to check whether the blur is coming from the back of the eye rather than the front. In practice, this is one of the classic reasons a patient says, “The pain is gone, but I still don’t see well.” (Mayo Clinic)
Corneal swelling, surface dryness, and deposits can also blur the view
The cornea is the clear front window of the eye. During inflammation, it may become affected in several ways. Some patients develop mild corneal edema, meaning swelling that makes the vision look hazy. Others have keratic precipitates, which are inflammatory deposits on the inner surface of the cornea. Some also experience a dry, irritated surface from frequent drops or preservative exposure, and that can create fluctuating blur that comes and goes with blinking. (NCBI)
Patients sometimes notice that the blur is worse at certain times of day or improves briefly after blinking or using lubricant drops. That pattern leans more toward surface dryness than deep active inflammation, although both can exist together. It is worth mentioning this to your doctor because the answer is not always “more steroid.” Sometimes the surface of the eye needs help too. (American Academy of Ophthalmology)
Why “feels better” does not always equal “healed”
This is a key clinical lesson. Symptoms tell us part of the story. Examination tells us the rest.
Uveitis follow-up is not just a formality. Your ophthalmologist is checking whether the number of inflammatory cells in the eye is actually decreasing, whether synechiae are forming, whether the eye pressure is safe, and whether the retina remains healthy. Topical corticosteroids are standard treatment for anterior uveitis, but they need careful monitoring because undertreated inflammation can lead to lasting damage, while overtreatment can cause steroid-related complications. (NCBI)
This balance is why patients are told not to stop steroid drops suddenly unless instructed. Inflammation may rebound if treatment is reduced too quickly. On the other hand, continuing steroid drops for too long without supervision is also unsafe because of the risk of pressure rise and other side effects. (NNUH)
A practical way to think about blurry vision after starting treatment
In clinic, I often explain it this way.
Blur from uveitis treatment usually falls into three buckets.
The first is expected blur from treatment itself. This is commonly caused by dilating drops and usually affects focusing, especially for reading or screen work. It may also be accompanied by glare and light sensitivity. The eye may actually be healing normally. (Oxford University Hospitals)
The second is healing blur from inflammation that is improving but not yet gone. The eye is less red and less painful, but there are still inflammatory cells, protein, or mild tissue changes inside. Vision often improves, but more slowly. (NCBI)
The third is warning-sign blur. This includes worsening vision, new floaters, increasing light sensitivity, increasing redness, headache, nausea, halos around lights, or persistent central smudging. That pattern makes us worry about still-active inflammation, retinal swelling, pressure rise, corneal edema, or another complication. (Mayo Clinic)
Red flags that deserve urgent review
Some changes should not wait for the next routine appointment.
If vision suddenly worsens, if new floaters appear quickly, if pain returns, if redness increases again, or if you develop severe light sensitivity, contact your eye doctor promptly. The same applies if you notice halos around lights, marked headache, nausea, or a sense that the eye is rapidly becoming more blurred rather than slowly improving. These symptoms can be associated with active inflammation or raised eye pressure and need examination, not guesswork. (NCBI)
Even when the symptoms are milder, persistent blur that is not improving as expected is worth discussing. Uveitis is one of those conditions where a reassuring exam is far more useful than reassurance based only on symptoms. (Mayo Clinic)
What your ophthalmologist may check at the follow-up visit
Patients sometimes feel discouraged when they are asked to come back frequently. In reality, those visits are how we separate normal healing from trouble.
Your doctor may check your vision, pupil, eye pressure, the number of inflammatory cells in the anterior chamber, the clarity of the cornea, and whether the back of the eye looks healthy. In some cases, additional testing such as OCT or retinal imaging is needed. The aim is not only to confirm that the drops are working, but also to make sure they are the right treatment, at the right dose, for the right part of the eye. (Mayo Clinic)

What patients should and should not do at home
The most useful thing you can do is use the drops exactly as prescribed and attend follow-up appointments. Do not stop steroid drops just because the eye feels better, and do not taper them on your own. Sudden reduction can allow the inflammation to flare again. (NNUH)
It is also wise to keep track of the quality of the blur. Is it mainly near vision? Is it present all day or only after drops? Is it improving a little every day? Are there new floaters or distortion? This kind of detail helps your ophthalmologist work out whether the blur is more likely from dilation, surface irritation, lingering inflammation, or retinal involvement. That observation is often more helpful than simply saying, “It’s still blurry.”
Wear sunglasses outside if light sensitivity is troublesome. Be careful with driving if the eye is dilated or your focus is poor. And do not self-medicate with leftover steroid drops from an old episode unless your ophthalmologist has specifically instructed you to do that. Different causes of red eye can look similar, and steroids can worsen some infections. (Moorfields Eye Hospital)
The reassuring truth and the honest truth
The reassuring truth is that blurry vision after starting steroid drops for uveitis is common, and it does not automatically mean your treatment is failing. There are many ordinary reasons for foggy vision early in the course, especially if you are using dilating drops or if the inflammation is improving more slowly than the pain. (Moorfields Eye Hospital)
The honest truth is that blurry vision should still be taken seriously. Uveitis can damage vision if it remains active or if complications develop, and steroid treatment itself requires supervision. The eye may look better on the surface while deeper structures still need attention. (NCBI)
So the best answer to the question in the title is this: blurred vision after starting steroid drops may represent healing, it may be an expected treatment side effect, or it may be a sign that your uveitis is still active. The difference cannot be judged safely from symptoms alone. It needs an eye examination. (Mayo Clinic)
When to see your doctor
If your blur is mild and your doctor already warned you that the dilating drops would affect your focus, the symptom may be expected. But if your vision is not gradually improving, if it worsens, or if you have new floaters, pain, redness, halos, headache, nausea, or worsening light sensitivity, you should contact your ophthalmologist sooner rather than later. (Oxford University Hospitals)
For anyone being treated for uveitis, the safest mindset is this: comfort improving is encouraging, but vision is the score we protect.
Call to action
If you are being treated for uveitis and your vision is still foggy, do not panic, but do not ignore it either. Book your follow-up eye examination as advised, and seek earlier review if the blur is worsening or accompanied by new symptoms. A timely check can confirm that the eye is healing well, adjust treatment if inflammation is still active, and protect your long-term vision.
References
American Academy of Ophthalmology, “What Are Dilating Eye Drops?” (American Academy of Ophthalmology)
Mayo Clinic, “Uveitis: Symptoms and causes.” (Mayo Clinic)
Mayo Clinic, “Uveitis: Diagnosis and treatment.” (Mayo Clinic)
National Eye Institute, “Uveitis.” (National Eye Institute)
NCBI Bookshelf, StatPearls, “Uveitis.” (NCBI)





