
If you were told you have uveitis and then heard terms like HLA-B27 or Behçet’s disease for the first time, it can feel alarming. In many people, uveitis is the first clue that the immune system may be involved, but it does not automatically mean you have a lifelong autoimmune disease. HLA-B27 is a genetic marker, not a diagnosis. Behçet’s is a specific inflammatory condition with eye, mouth, skin, and sometimes blood vessel or joint symptoms. The key next step is a focused medical workup, not panic.
What HLA-B27, Behçet’s, and Other Autoimmune Links Really Mean After a Uveitis Diagnosis
A uveitis diagnosis often raises two fears at once. The first is, “Will this affect my vision?” The second is, “Does this mean something bigger is wrong with my immune system?” Both are reasonable questions.
Uveitis means inflammation inside the eye. It can cause eye pain, redness, light sensitivity, floaters, blurred vision, and in some cases vision loss if treatment is delayed. It can affect one eye or both, and it may happen once, return in flares, or become long term. The National Eye Institute notes that uveitis sometimes happens because the immune system attacks healthy tissue, but it can also be linked to infections or other causes.
That is why hearing terms like HLA-B27, Behçet’s disease, sarcoidosis, psoriasis, ankylosing spondylitis, or inflammatory bowel disease after an eye flare is not unusual. The eye can sometimes be the first place the body “shows” inflammation. In other words, yes, uveitis can be the first autoimmune clue for some people. But just as importantly, it is not always the first clue, and it is not always an autoimmune story. Sometimes the cause is infectious. Sometimes it remains unclear even after careful testing. And sometimes the eye inflammation is treated successfully even when no exact cause is ever found.
Why uveitis sometimes leads to a broader health workup
When an ophthalmologist diagnoses uveitis, they do not only look at the eye. They also look for patterns. Which part of the eye is inflamed? Is it the front part of the eye, called anterior uveitis, or the back part, or all of it? Is the inflammation sudden and painful, or quieter and chronic? Is it in one eye or both? Has it happened before? These details matter because certain patterns are more strongly linked to specific systemic diseases.
For example, anterior uveitis is the most common type. EyeWiki from the American Academy of Ophthalmology notes that anterior uveitis makes up the large majority of uveitis cases, and HLA-B27-associated disease is a classic link, especially when the inflammation is acute and recurrent. The same source notes that broad, untargeted “uveitis survey” testing is discouraged because it often has low value; testing is usually more useful when it is guided by the eye findings and the patient’s symptoms. That is an important point for patients: a good workup is usually focused, not random.

What HLA-B27 actually means
HLA-B27 is a genetic marker. It is part of a group of molecules the immune system uses to help recognize what belongs in the body and what does not. A positive HLA-B27 test does not mean you “have an autoimmune disease” by itself. It also does not mean that uveitis will definitely keep coming back. It simply means you have a gene variant that is associated with a higher chance of certain inflammatory conditions.
This distinction matters. Mayo Clinic states that many people who have the HLA-B27 gene never develop ankylosing spondylitis, even though the gene raises risk. So if your test is positive, the result should be read as a clue, not a verdict. It tells your doctors where to look more carefully, especially if you also have symptoms such as inflammatory back pain, morning stiffness, heel pain, swollen joints, psoriasis, diarrhea with blood, or a history of reactive arthritis.
In eye care, HLA-B27 is especially relevant because about half of acute anterior uveitis cases are associated with this marker, according to current AAO EyeWiki material. That does not mean half of all people with a positive HLA-B27 test get uveitis. It means that among patients who come in with that specific eye inflammation pattern, HLA-B27 is common enough that doctors think about it early.
Many patients worry that a positive HLA-B27 result means they must already have ankylosing spondylitis. That is not true. Some patients with HLA-B27-associated uveitis do have a known spondyloarthritis diagnosis. Others are diagnosed later after more history, imaging, or rheumatology review. And some never develop a defined systemic disease at all. The point of testing is not to label you too quickly. The point is to catch a pattern early if it is there.
When uveitis is the first clue to a spondyloarthritis-type condition
The autoimmune group most classically linked to HLA-B27-related uveitis is the spondyloarthritis family. This includes ankylosing spondylitis and related inflammatory conditions. These diseases often affect the spine, sacroiliac joints, heels, and other joints, and can also be linked with psoriasis, bowel inflammation, or inflammation after certain infections. MedlinePlus lists ankylosing spondylitis, psoriasis, reactive arthritis, and ulcerative colitis among autoimmune conditions associated with uveitis.
Sometimes the eye flare happens before the back symptoms are recognized as abnormal. A patient may think, “I just have stiffness when I wake up,” or “I’ve always had back pain,” not realizing the pattern suggests inflammation rather than muscle strain. Mayo Clinic notes that uveitis is one of the most common complications of ankylosing spondylitis and that the symptoms can include sudden eye pain, redness, light sensitivity, and blurry vision. In practice, that means a first uveitis episode may lead your doctor to ask questions you did not expect, such as whether back pain improves with movement, whether your heels hurt, or whether a close relative has psoriasis or inflammatory bowel disease.
This is why patients sometimes feel their visit becomes “about more than the eye.” The eye specialist is not losing focus. They are doing exactly what good uveitis care requires: connecting eye findings to the rest of the body.
What Behçet’s disease means, and why it is different
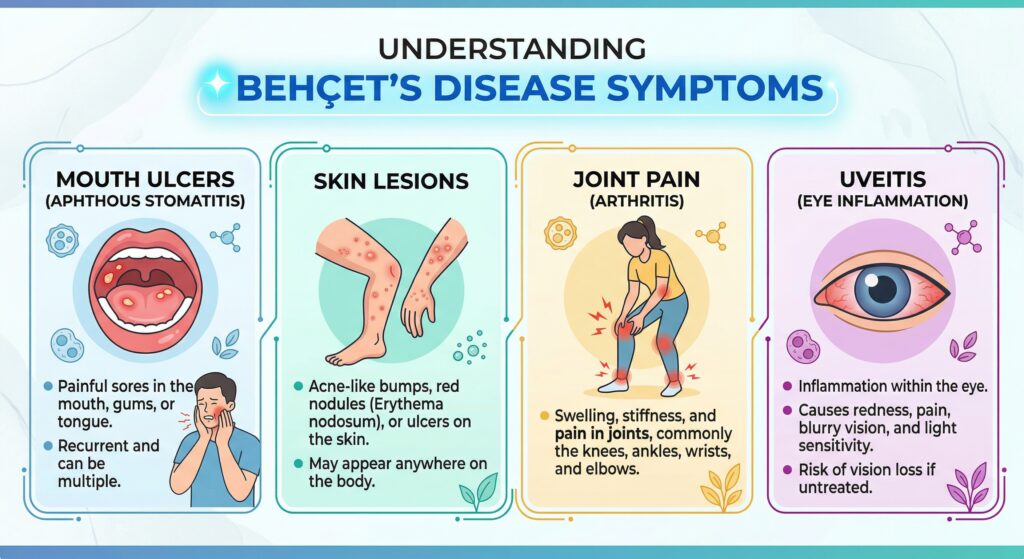
Behçet’s disease is different from a simple HLA-B27 result. HLA-B27 is a marker. Behçet’s is a specific inflammatory disease. It can affect the eyes, mouth, skin, joints, blood vessels, gut, and nervous system. NHS guidance notes that eye inflammation in Behçet’s can occur suddenly and may cause painful red eyes, light sensitivity, floaters, blurred vision, and sudden vision loss. It also notes that many people with Behçet’s have recurrent mouth ulcers and may have genital ulcers, skin lesions, joint symptoms, or blood vessel problems.
For patients, the practical message is this: Behçet’s is usually not diagnosed from the eye alone. Doctors look for the whole pattern. A person with recurrent uveitis plus repeated mouth ulcers, genital sores, acne-like or tender skin lesions, joint pain, and sometimes unusual clotting problems raises a different level of suspicion than someone with a single episode of anterior uveitis and no other symptoms.
Behçet’s can be serious because it may involve more than one organ system, and the eye disease can threaten sight if not treated quickly. NHS guidance emphasizes that early, appropriate treatment lowers the chance of permanent vision loss, and that care is often coordinated across specialists. That team may include ophthalmology, rheumatology, dermatology, and sometimes neurology or vascular medicine depending on the symptoms.
Other autoimmune links doctors may think about
HLA-B27 and Behçet’s often get attention because they are memorable names, but they are not the only possibilities. The National Eye Institute lists multiple autoimmune diseases associated with uveitis, including ankylosing spondylitis, Behçet’s disease, lupus, multiple sclerosis, psoriasis, rheumatoid arthritis, sarcoidosis, ulcerative colitis, and Vogt-Koyanagi-Harada disease. MedlinePlus lists several overlapping conditions as well.
The exact list your doctor considers depends on how the uveitis looks and what other symptoms you have. For example, bowel symptoms may push the workup toward inflammatory bowel disease. Skin plaques may point toward psoriasis. Lung symptoms, abnormal chest imaging, or certain exam findings may raise suspicion for sarcoidosis. A very specific pattern in the back of the eye may suggest something else entirely. This is why two patients with “uveitis” can end up having very different blood tests, scans, or referrals.
It is also important to remember that not all causes are autoimmune. NEI and MedlinePlus both note infectious causes such as shingles, syphilis, toxoplasmosis, histoplasmosis, and cytomegalovirus. That matters because the treatment approach can change significantly if infection is involved. Steroids are often central in noninfectious uveitis, but in infectious uveitis they may need to be combined with or preceded by antimicrobial treatment.
What testing after a uveitis diagnosis usually involves
Patients often ask, “What tests should I have?” The honest answer is that there is no one standard panel for everyone. Mayo Clinic states that if an underlying condition may be causing your uveitis, your eye specialist may refer you for a general medical exam and laboratory tests. The key word is may. Testing should match the pattern, not just the fear.
If your eye findings suggest acute recurrent anterior uveitis, your doctor may order HLA-B27 testing. If sarcoidosis is on the list, chest imaging and other targeted tests may be more relevant. If infection is possible, infectious workup may come first. Current AAO material specifically warns against broad, non-targeted testing because it often has low predictive value and rarely changes management. That is reassuring in a way: more tests do not always mean better care. Smarter tests do.
The medical history is often just as important as the blood work. A focused set of questions can reveal patterns that patients have never connected before: chronic low back stiffness, heel pain, psoriasis, mouth sores, genital ulcers, chronic diarrhea, cough, skin nodules, previous sexually transmitted infections, recent infections, or a family history of autoimmune disease. These details can turn a vague lab result into a meaningful diagnosis.
What treatment means when an autoimmune link is suspected
Many patients assume that once an autoimmune link is found, the eye treatment changes completely. In reality, the first goal is still to control the inflammation in the eye quickly and safely. NEI notes that treatment often includes steroids, commonly as eye drops, but sometimes as pills, injections, or implants depending on where the inflammation is and how severe it is. Mayo Clinic similarly notes that treatment aims to reduce swelling in the eye and elsewhere in the body if needed.
If the uveitis is tied to a systemic inflammatory disease, long-term care may also include medicines that calm the immune system more broadly. In Behçet’s disease, NHS notes that there is no cure, but treatments can help control symptoms and reduce the risk of serious complications, often with input from several specialists. That is why a patient might start with an urgent eye treatment plan and later also meet a rheumatologist or immunologist.
The big idea is that eye treatment and body treatment are not competing goals. They are usually parts of the same strategy. Save vision now, reduce recurrence risk later, and identify whether there is a treatable systemic disease underneath.
Questions patients should ask after hearing “HLA-B27” or “Behçet’s”
After a uveitis diagnosis, it helps to ask practical questions instead of trying to decode everything online in one night.
Ask whether your uveitis pattern fits a common autoimmune association or whether infection is still being considered. Ask whether the HLA-B27 result is being used as a clue or whether there are already enough signs to suspect a defined spondyloarthritis. Ask whether your symptoms outside the eye suggest Behçet’s disease or another inflammatory condition. Ask whether you need a rheumatology referral now, or only if the inflammation recurs. And ask what warning symptoms mean you should seek urgent care again. Mayo Clinic suggests similar questions for patients with uveitis, including the likely cause, what tests are needed, whether the condition may be temporary or long lasting, and what treatments are recommended.
When to worry, and when not to panic
It is appropriate to take uveitis seriously. NEI states that uveitis can cause vision loss if it is not treated and that symptoms such as blurry vision, floaters, pain, red eye, and light sensitivity should prompt urgent eye evaluation. Behçet’s-related eye inflammation can also be sudden and severe. So do not downplay new symptoms.
At the same time, do not assume the worst from a single word on a lab report. A positive HLA-B27 does not equal a confirmed autoimmune disease. Even when uveitis is the first clue, the diagnosis of a systemic condition usually depends on the larger pattern over time, not one test alone. And even when no clear cause is found, treatment can still work very well.
That balance is important. Urgent, yes. Hopeless, no.
A sensible next-step plan after diagnosis
If you have just been diagnosed with uveitis, the most helpful mindset is this: treat the eye flare promptly, keep follow-up appointments, and let your doctors look for patterns rather than jumping to conclusions yourself.
Keep a note of symptoms outside the eye. Mouth ulcers, genital ulcers, persistent back stiffness, swollen joints, skin rashes, bowel changes, or repeated flares are all worth mentioning. Bring old records if you have them. If your ophthalmologist recommends blood tests or referral to a rheumatologist, that is not because they are certain you have a systemic disease. It is because uveitis can be a window into immune health, and catching the right diagnosis early can protect both sight and overall health.
When to see a doctor urgently
Any new eye pain, redness, sudden blur, floaters, or light sensitivity deserves prompt attention. NEI advises seeing an eye doctor right away for these symptoms because untreated uveitis can lead to vision loss. If you already carry a diagnosis of Behçet’s disease or recurrent uveitis, do not wait to “see if it settles.” Eye flares can escalate quickly.
Final takeaway
For many people, a uveitis diagnosis is the first time they hear the language of autoimmunity. That can be frightening, but it helps to translate the terms clearly.
HLA-B27 means “possible immune pattern,” not “final diagnosis.”
Behçet’s means “specific inflammatory disease,” not just a lab result.
Uveitis can be the first autoimmune clue, but it can also be caused by infection or remain isolated to the eye.
The right response is not panic. It is careful follow-up, targeted testing, and coordinated care.
If you have had a recent uveitis flare, book a detailed follow-up with your ophthalmologist and discuss whether your eye pattern suggests HLA-B27-associated disease, Behçet’s disease, or another systemic cause. A timely eye exam and the right medical history can make the difference between a temporary scare and a missed diagnosis.
References
- National Eye Institute. Uveitis.Thank you.
- American Academy of Ophthalmology EyeWiki. HLA-B27 Associated Acute Anterior Uveitis.
- American Academy of Ophthalmology EyeWiki. Acute Anterior Uveitis.
- NHS. Behçet’s disease: Symptoms.
- Mayo Clinic. Uveitis: Diagnosis and treatment.





