Floaters, blurry vision, halos, and light sensitivity are not always harmless. Sometimes they come from common age-related vitreous changes, but they can also signal uveitis, a retinal tear or detachment, or even a sudden pressure rise from angle-closure glaucoma. A painful red eye is not required for a serious problem. Intermediate or posterior uveitis can be mostly painless and still threaten sight. New or sudden symptoms, flashes of light, a curtain or shadow, marked light sensitivity, or fast worsening blur need urgent eye care the same day.
Uveitis or Retina Problem? How to Tell Whether Floaters, Blur, or Light Sensitivity Need Urgent Eye Care
Patients often ask a very reasonable question: “Are these floaters and blurry vision just normal, or is something wrong?” It is one of the most important questions in eye care, because the answer can range from “this is common and not dangerous” to “you need urgent treatment today.”
What makes this confusing is that different eye problems can produce similar symptoms. A person with simple age-related vitreous changes may notice floaters. Someone with posterior vitreous detachment may notice a sudden burst of new floaters and flashes. A person with uveitis may notice floaters and blur with light sensitivity. A person with retinal detachment may describe black specks, flashing lights, or a curtain coming over part of the vision. Another person may complain mainly of halos around lights and blurred vision, which can point more toward corneal swelling or angle-closure glaucoma than a retinal problem.
The key message is simple: symptoms have to be interpreted in context. There is no single symptom that always tells the whole story. But there are patterns that help us decide what might be going on and how urgently you should be examined.
Why this topic matters
Many people have heard that uveitis causes a painful red eye. That is true for many cases of anterior uveitis, which affects the front part of the eye. But it is not true for every type. Intermediate uveitis often causes floaters and blurred vision. Posterior uveitis can cause decreased vision and floaters, and it is often painless and slower to develop. That means serious inflammation can be present even when the eye does not look dramatically red from the outside.
That is exactly why patients can be falsely reassured. They may think, “It can’t be serious because it doesn’t hurt much,” or “My eye isn’t red.” Unfortunately, that is not always safe thinking. Some retinal problems are also painless, including retinal detachment, which is an emergency.
First, what do these symptoms actually mean?
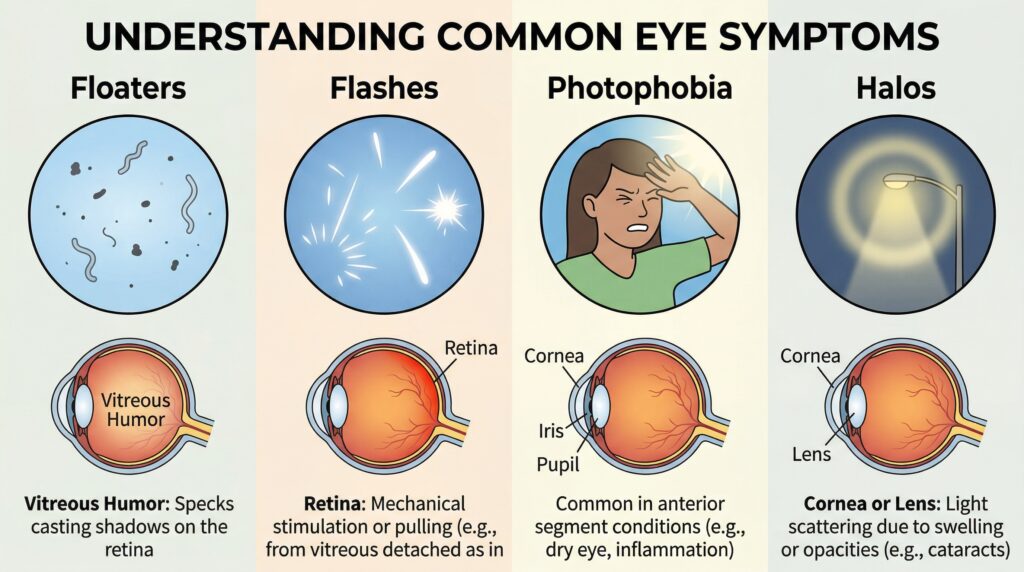
Floaters
Floaters are tiny specks, threads, cobwebs, or shadowy shapes that drift through your vision. Many floaters are caused by age-related changes in the vitreous, the gel inside the eye. They can be annoying but not dangerous. However, a sudden increase in floaters can also happen when the vitreous pulls away from the retina, and in some people this can create a retinal tear or lead to retinal detachment. Uveitis can also cause floaters because inflammatory cells and debris enter the vitreous.
Blurry vision
Blurred vision is very nonspecific. It may come from inflammation, retinal swelling, retinal tears or detachment, corneal swelling, glaucoma, cataract, dry eye, or even just an outdated glasses prescription. In uveitis, blur may come from active inflammation or complications such as macular edema. In retinal detachment, blur often worsens as more retina lifts away.
Light sensitivity
Light sensitivity, also called photophobia, is common in anterior uveitis because the inflamed iris and ciliary body react painfully to light. But photophobia can also occur with corneal disease and some other inflammatory conditions. It is less classic for a retinal tear or detachment by itself. So when a patient has prominent photophobia, especially with blur and discomfort, inflammation in the front of the eye moves higher on the list. Still, posterior or intermediate uveitis may not have dramatic pain or redness, which is why symptoms must be assessed carefully rather than by a simple checklist.
Halos around lights
Halos are another symptom patients often describe vaguely. They may say lights look smeared, ringed, foggy, or rainbow-colored. Halos are not the classic symptom of a retinal tear or posterior uveitis. They are more often linked with problems affecting the cornea or eye pressure, including acute angle-closure glaucoma, where people may also have severe eye pain, redness, headache, nausea, and blurred vision. Cataract and some corneal conditions can also cause halos.
When symptoms are more likely to suggest uveitis
Uveitis means inflammation inside the eye. It can affect the front of the eye, the middle, the back, or multiple areas. Symptoms vary depending on where the inflammation is located.
Anterior uveitis more often causes pain, redness, blurry vision, and light sensitivity. This is the form many people picture when they hear the word uveitis.
Intermediate uveitis commonly causes floaters and blurred vision. It may not cause much redness or pain. Posterior uveitis often causes decreased vision and floaters and is usually painless. It can develop more slowly and may be more damaging because patients do not always seek care quickly.
So, what symptom pattern should make you think about uveitis?
A gradual or subacute change rather than a dramatic instant event can fit uveitis. Floaters plus blur can fit uveitis, especially when there is also light sensitivity or a history of autoimmune or inflammatory disease. Symptoms may affect one eye or both. The eye may look only mildly red, or even look nearly normal to a family member looking at it casually.
Doctors also think about uveitis more strongly when there is a past history of uveitis, inflammatory bowel disease, psoriasis, ankylosing spondylitis, sarcoidosis, certain infections, or unexplained repeated flares of eye inflammation. Not every patient has an underlying illness, but these associations matter. Mayo Clinic notes that uveitis may be related to infection, injury, or autoimmune and inflammatory disease, and sometimes no clear cause is found.
When symptoms are more likely to suggest a retinal problem
s become more concerning when the story is sudden. A retinal tear or detachment often causes a new shower of floaters, flashes of light, worsening side vision, or a shadow or curtain over part of the visual field. Retinal detachment is typically painless. That is one reason people delay care. They may expect severe pain if something is truly wrong, but retinal detachment can threaten sight without hurting.
A simple posterior vitreous detachment can also cause sudden floaters and flashes. In many cases it is not dangerous by itself, but the only way to know whether it has caused a retinal tear is to have a dilated eye exam. The National Eye Institute specifically notes that symptoms of vitreous detachment need prompt examination because more serious eye problems can look similar at first.
This is an important practical point for patients: “I just got new floaters” is not something to self-diagnose. Many cases turn out to be benign, but some are not, and the early symptoms can overlap.
A symptom-by-symptom comparison
Floaters alone
A few long-standing floaters that have not changed much are often less concerning. A sudden increase in floaters is different. That can happen in posterior vitreous detachment, retinal tear, retinal detachment, bleeding inside the eye, or uveitis. The more sudden and dramatic the change, the more urgent the exam.
Floaters plus flashes
This pattern raises concern for vitreous traction on the retina and possible retinal tear or detachment. It is not a symptom to watch casually for several days without advice. Same-day or very prompt assessment is usually appropriate.
Floaters plus photophobia
This combination makes inflammation, especially uveitis, more concerning. It does not rule out retinal disease, but photophobia shifts the conversation toward inflammatory or anterior segment causes.
Blurred vision plus a curtain, shadow, or missing side vision
This is a retinal emergency until proven otherwise. Patients describe it in many ways: “a dark veil,” “a shade,” “part of the side vision went gray,” or “there is a black area I can’t see through.” These are classic retinal detachment warning signs.
Halos plus pain, redness, nausea, or headache
This pattern is less typical for retina or posterior uveitis and more worrisome for acute angle-closure glaucoma or a corneal problem. Acute angle closure needs urgent treatment.
Blur without pain or redness
This is where mistakes happen. Many patients assume painless blur cannot be serious. But posterior uveitis, intermediate uveitis, vitreous problems, macular disease, diabetic retinopathy, and retinal detachment can all be painless. Painless does not mean harmless.
Why the “red painful eye” rule is not enough
A painful red eye is an important clue, but it is not a reliable screening tool for all serious disease. Anterior uveitis often does cause redness and pain. Posterior and intermediate uveitis may not. Retinal detachment is usually painless. Vitreous detachment can be painless. Some serious macular and retinal conditions cause distortion or blur with no redness at all.
This is why I tell patients not to use the mirror as their main diagnostic tool. Looking at the eye from the outside is not enough to judge whether the retina is attached, whether inflammatory cells are floating in the vitreous, or whether the macula is swollen. Those questions require an eye examination.
How an ophthalmologist tells the difference
The most important first step is the history. We ask when the symptoms began, whether they were sudden or gradual, whether one eye or both are affected, whether you see flashes, whether part of the vision is blocked, whether light hurts, whether you have pain, and whether you have had trauma, recent surgery, diabetes, or prior eye inflammation. Mayo Clinic notes that a full exam for floaters usually includes dilation to allow the doctor to examine the vitreous and the retina properly.
After that, the exam often includes checking vision, eye pressure, the front of the eye with a slit lamp, and a dilated retinal exam. If uveitis is suspected, the doctor looks for inflammatory cells, flare, keratic precipitates, vitreous haze, retinal vasculitis, or choroidal lesions, depending on the suspected type. If a retinal tear or detachment is suspected, the peripheral retina must be examined carefully, often through dilated pupils. Some patients also need retinal imaging such as OCT or photographs, and selected patients need blood tests or referral to evaluate a possible underlying inflammatory or infectious cause of uveitis.
Treatment depends on the cause, not just the symptom
This is another reason self-treatment is risky. “Floaters” are not the diagnosis. “Blur” is not the diagnosis. Those are symptoms.
If the problem is uncomplicated age-related vitreous change, treatment may not be needed. If the problem is posterior vitreous detachment, careful retinal examination and follow-up are important to make sure no tear develops. If the problem is retinal detachment, treatment may involve laser or surgery, and time matters because delay increases the risk of permanent vision loss.
If the problem is uveitis, treatment often includes steroid eye drops, steroid injections, oral medicines, or other treatment depending on where the inflammation is and what caused it. The National Eye Institute and the AAO both note that steroids are commonly used to reduce eye inflammation, but the exact approach depends on the type and cause. Some cases also need treatment for infection or longer-term immune control.
This is why using leftover steroid drops without a diagnosis can be unsafe. Steroids can be helpful in true uveitis, but they can worsen some infections and may complicate glaucoma or other conditions. Treatment should follow examination, not guesswork.
When symptoms need urgent eye care
Patients do not need to memorize every diagnosis. They do need to recognize danger signs.
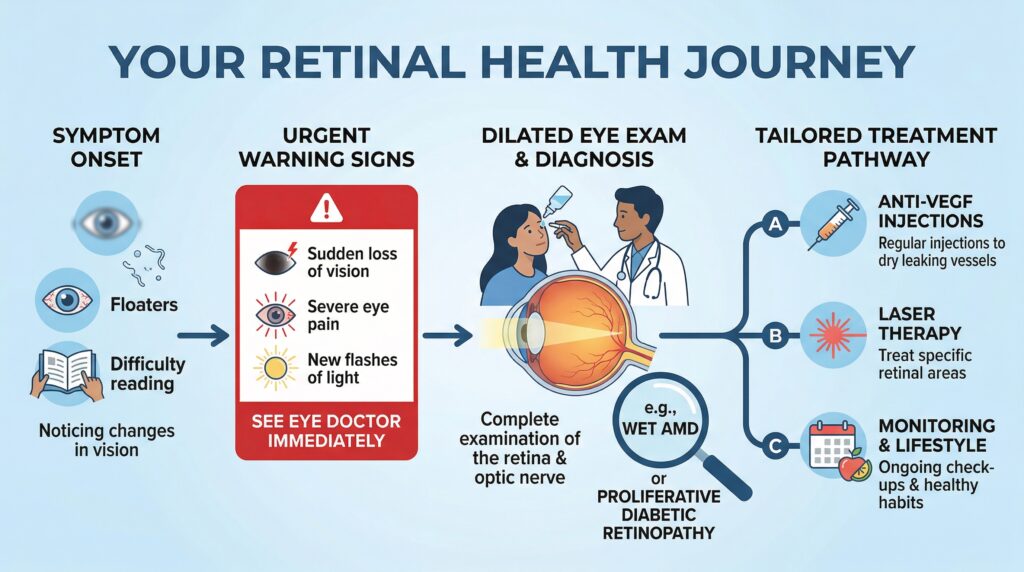
You should seek urgent, same-day eye care for a sudden shower of new floaters, flashes of light, a curtain or shadow in the vision, quickly worsening blur, major light sensitivity, significant eye pain, or halos with a red painful eye. Retinal detachment, retinal tear, acute angle-closure glaucoma, and active uveitis can all threaten vision if treatment is delayed.
Even if the eye is not red and does not hurt, you should not ignore sudden new visual symptoms. Posterior uveitis and retinal problems can be subtle externally but serious internally.
Practical advice for patients and families
The safest rule is this: do not label new visual symptoms as “normal” just because you have heard floaters are common with age. Some are. Some are not. The urgency depends on the pattern.
A few stable floaters you have had for years are different from a burst of new floaters today.
Mild blur after a long screen day is different from blur plus flashes, photophobia, or a field defect.
A sore, light-sensitive eye is different from a truly painless retina problem, but both can still be urgent.
And perhaps most importantly, posterior or intermediate uveitis may not give you the classic painful red eye you expect. That is why patients with floaters and blur should not be dismissed just because the outside of the eye “looks fine.”
When to see a doctor
See an ophthalmologist urgently if you have any new or sudden floaters, flashes, a curtain or shadow, rapid worsening of vision, major light sensitivity, or halos with pain or redness. If you cannot reach an eye clinic quickly and you have a curtain over vision, severe pain, or fast vision loss, go to emergency care.
If your symptoms are milder but persistent, such as ongoing blur, recurrent floaters, or discomfort with light, you still need a timely eye exam. The goal is not only to diagnose emergencies but also to catch treatable inflammation or retinal disease before lasting damage occurs.
Final takeaway
Patients are right to ask whether floaters, blur, halos, or photophobia are “normal.” Sometimes they are not dangerous. But they are never symptoms to interpret casually when they are new, sudden, or getting worse.
If I had to give one bottom-line rule, it would be this: sudden floaters, flashes, field loss, or a curtain suggest a retinal emergency until proven otherwise; floaters with blur and light sensitivity raise concern for uveitis, even if there is little redness or pain; halos with pain and redness raise concern for acute pressure-related disease. In all of these situations, prompt examination protects vision.
Book an appointment with an ophthalmologist promptly if you notice these symptoms, especially if they are new, sudden, or worsening. A dilated eye exam is often the step that makes the difference between reassurance and sight-saving treatment.
References
- American Academy of Ophthalmology, “What Is Uveitis?”
- National Eye Institute, “Retinal Detachment.”
- National Eye Institute, “Vitreous Detachment.”
- Mayo Clinic, “Retinal detachment: Symptoms and causes.”
- Mayo Clinic, “Uveitis: Symptoms and causes.”