
Posterior uveitis is inflammation at the back of the eye, affecting the retina and nearby tissues that are essential for vision. Unlike the more familiar “red, painful eye,” this form often causes blurred vision, floaters, and gradual vision loss with little or no pain. That is why people sometimes ignore it until damage has already begun. Causes range from infections to autoimmune disease, and some cases have no clear trigger. Early diagnosis, retinal imaging, and the right treatment are important because untreated inflammation can scar the retina and permanently reduce sight.
Posterior Uveitis Explained: Why Retina Inflammation Can Cause Vision Loss Without Much Pain
When patients hear the word “uveitis,” many imagine a bright red, painful eye that becomes impossible to ignore. That image is true for some forms of uveitis, especially anterior uveitis, which affects the front part of the eye. But posterior uveitis is different. It affects the back of the eye, where the retina and choroid sit, and it often behaves quietly. Instead of dramatic redness or severe pain, patients may notice that vision is becoming hazy, floaters are appearing, or reading is suddenly harder. Sometimes the change is slow enough that people adapt to it before realizing something is wrong. (National Eye Institute)
That quiet pattern is exactly what makes posterior uveitis important. The retina is the light-sensing tissue of the eye. It works a little like the sensor in a camera, turning light into signals that the brain understands as vision. If inflammation affects this tissue, the result is not just discomfort. It can directly affect the quality of what you see. In other words, posterior uveitis may be less painful than some other eye inflammations, but it can be more dangerous to sight. Moorfields notes that posterior uveitis often causes decreased vision and floaters, tends to develop more slowly, and can be more damaging to the eye than other types of uveitis. (Moorfields Eye Hospital)
What exactly is posterior uveitis?
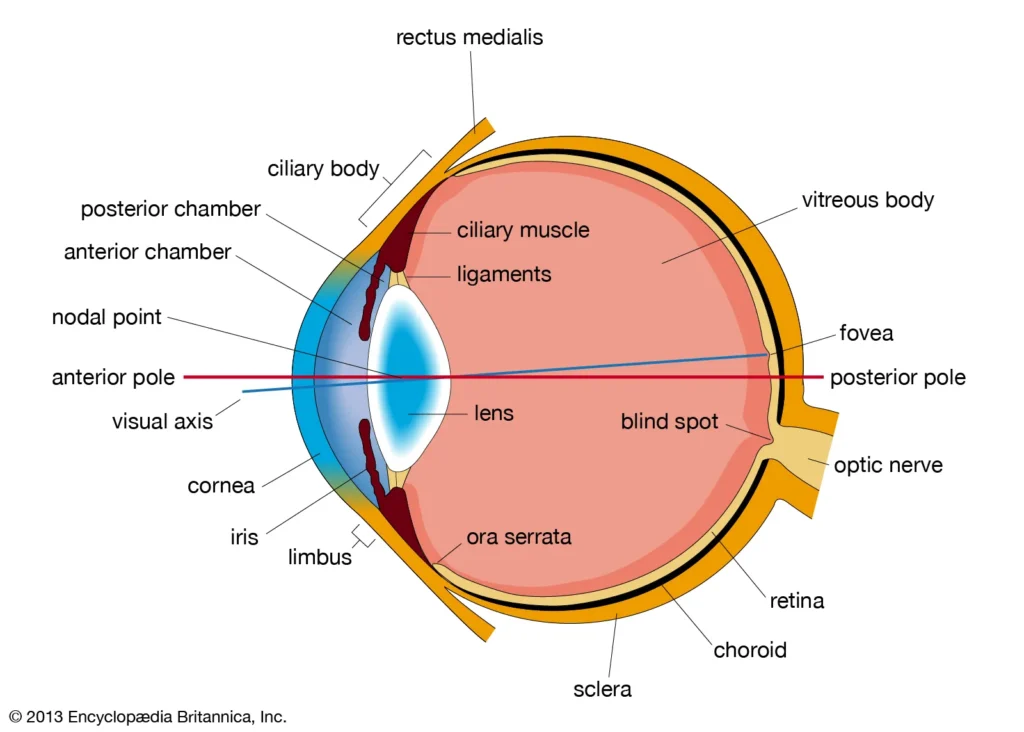
The eye has several layers. One important layer is the uvea, which includes the iris at the front, the ciliary body in the middle, and the choroid at the back. Posterior uveitis refers to inflammation involving the back part of the eye, especially the choroid and often the retina and retinal blood vessels as well. In real life, doctors may see inflammation in more than one structure at the same time, so posterior uveitis can overlap with retinitis, choroiditis, retinochoroiditis, vasculitis, or optic nerve inflammation. (National Eye Institute)
This is why the name can sound confusing. Patients may hear different words depending on which tissue looks most inflamed. But the key idea is simple: the inflammation is happening in the part of the eye responsible for fine, detailed vision. That is why symptoms may include blurred central vision, missing spots, reduced contrast, dim vision, distorted vision, or floating specks drifting across sight. Pain may be absent because the inflamed tissues at the back of the eye do not produce the same kind of obvious front-of-eye irritation seen in anterior uveitis. (National Eye Institute)
Why can vision drop without much pain?
This is the question that confuses many patients, and honestly, it is a very reasonable question. Most people assume that a serious eye problem must hurt. But the eye is not one single structure. Different parts of it behave differently. Inflammation at the front of the eye often causes pain, redness, and light sensitivity because the tissues there are richly supplied and easier to notice. Inflammation deeper in the eye can damage sight without triggering the same alarm signals. (American Academy of Ophthalmology)
Posterior uveitis can reduce vision in several ways. First, inflammatory cells and debris can spill into the vitreous, the gel that fills the eye, creating floaters and a cloudy view. Second, the retina itself can become inflamed, making it function poorly. Third, the macula, the small central area of the retina responsible for sharp reading vision, can swell. This swelling is called macular edema, and it is one of the main reasons patients lose vision from uveitis. Fourth, inflammation can affect retinal blood vessels or leave scars in the retina or choroid, causing longer-term or permanent visual loss. (Mayo Clinic)
Macular edema deserves special attention because it is common, treatable, and easy for patients to misunderstand. The word “edema” simply means swelling. When the macula swells, letters may look blurry, faces may lose clarity, and straight lines may seem less crisp. Research reviews describe uveitic macular edema as a common sight-threatening complication and a major cause of reduced visual acuity in posterior uveitis. In practical terms, this means a patient may say, “My eye is not painful, but I can’t read properly anymore.” That complaint should never be brushed aside. (PMC)
What symptoms should patients watch for?
The classic symptoms of posterior uveitis are not always dramatic. Many patients report floaters first. Floaters are those drifting spots, cobwebs, threads, or smoky shadows that move when the eye moves. Not every floater means inflammation, of course. Many floaters are harmless and related to normal changes in the vitreous. But when floaters are new, numerous, or associated with blurred vision, flashes, or reduced contrast, an eye exam becomes important. (Mayo Clinic)
Blurred vision is another common symptom. It may affect one eye or both. It may come on gradually or more quickly. Some people notice a gray patch, dimness, or trouble seeing in the center. Others feel that colors are less vivid or that one eye simply is not as sharp as the other. If the inflammation involves the peripheral retina, patients may not notice a problem until the disease is more advanced. That is one reason posterior uveitis can stay hidden for longer than anterior uveitis. (Moorfields Eye Hospital)
Pain, redness, and sensitivity to light can occur in uveitis overall, but they may be mild or absent in posterior disease. So the absence of pain does not reassure me as much as many patients expect. In eye care, “painless” does not always mean “harmless.” A painless drop in vision, especially with floaters, is still urgent enough to justify a proper dilated retinal examination. (National Eye Institute)
What causes posterior uveitis?
Posterior uveitis is not one disease with one cause. It is a pattern of inflammation that can happen for different reasons. Broadly, doctors think about infectious causes and non-infectious causes. This distinction matters because the treatment can be very different. Giving strong steroid treatment to someone with an untreated eye infection can worsen the problem, so identifying the cause is an essential part of management. (Mayo Clinic)
Non-infectious posterior uveitis may be linked to autoimmune or inflammatory diseases, where the immune system becomes overactive and attacks healthy tissues. In some patients, the inflammation is limited mainly to the eye. In others, it may be associated with a broader systemic condition. Even after careful testing, some cases remain idiopathic, which means no exact cause is found. That can be frustrating for patients, but it is common in uveitis care. (Mayo Clinic)
Infectious posterior uveitis can be caused by parasites, bacteria, viruses, or fungi, depending on the clinical setting and geography. Toxoplasmosis is a well-known cause of posterior segment inflammation. Tuberculosis and syphilis are also important because they can involve the eye and may need systemic treatment. Reviews of infectious uveitis emphasize that infections must always be considered, especially in posterior disease. (PMC)
Why is posterior uveitis sometimes missed?
There are several reasons. The first is symptom pattern. People often seek urgent help for pain and redness, but they may delay care for floaters or “slightly blurry” vision. The second is that the front of the eye may look fairly normal. Friends, family, or even the patient looking in a mirror may not see anything alarming. The third is that the disease can be intermittent or slowly progressive, which leads some people to wait and see. (Moorfields Eye Hospital)
Another reason is that floaters are common in everyday life, especially with aging or after a posterior vitreous detachment. Many floaters are benign. But because benign and serious causes can overlap in how they feel to the patient, examination is what separates one from the other. In posterior uveitis, the story often sounds subtle: “I thought I just needed new glasses,” or “I assumed it was eye strain.” That is exactly why patient education matters. (Mayo Clinic)
How is it diagnosed?
Diagnosis starts with a detailed history. A doctor will ask when the symptoms began, whether one or both eyes are involved, whether there is pain or light sensitivity, and whether there are any systemic symptoms such as joint pain, skin changes, fever, cough, mouth ulcers, or neurologic issues. Travel, infections, immune disease, medications, and prior episodes may all matter. Posterior uveitis is one of those conditions where the eye can provide clues to the rest of the body, and sometimes the rest of the body helps explain the eye. (National Eye Institute)
The eye examination itself is crucial. Visual acuity is checked, and the pupil is dilated so the doctor can look carefully at the vitreous, retina, choroid, optic nerve, and retinal vessels. This is not something that can be judged from symptoms alone. Two patients may both say “blurred vision,” but one may have mild vitreous inflammation while another has retinal vasculitis or macular edema. (National Eye Institute)
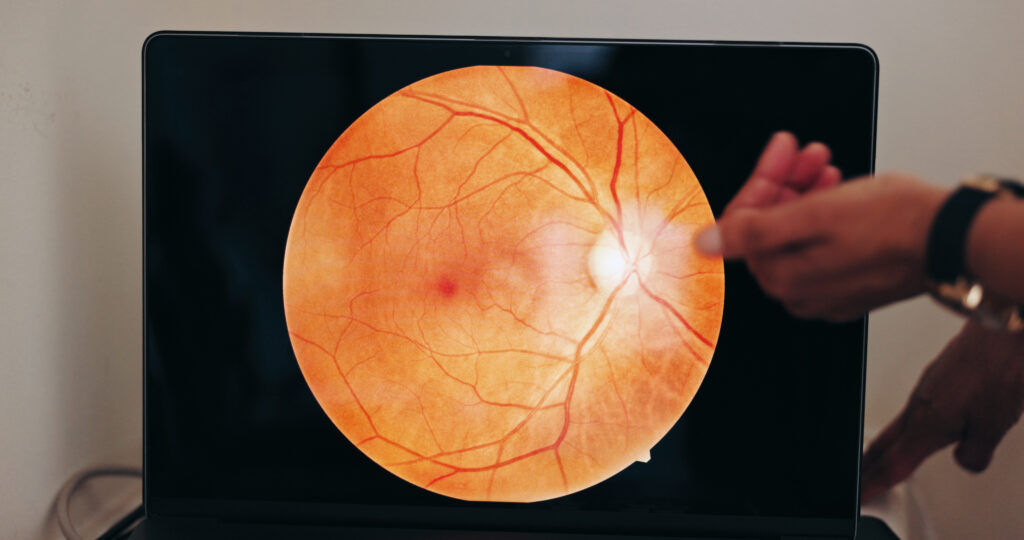
Retinal imaging is often where the diagnosis becomes clearer. Optical coherence tomography, or OCT, gives a cross-sectional scan of the retina and is very useful for detecting macular edema and monitoring treatment response. Fluorescein angiography, which uses dye to study retinal blood flow and leakage, remains an important tool in posterior uveitis, especially when vasculitis or hidden leakage is suspected. In selected cases, OCT angiography or indocyanine green angiography may also help. (PMC)
Blood tests or scans may be ordered, but good uveitis care is not just about ordering a long list of investigations. The best workup is targeted. Doctors choose tests based on the pattern seen in the eye and the patient’s history. That is one reason specialist input is often valuable. (doclibrary-rcht.cornwall.nhs.uk)

How is posterior uveitis treated?
Treatment depends on the cause, the location of inflammation, how severe it is, and whether one or both eyes are involved. The main goal is to stop inflammation quickly enough to protect the retina and preserve vision. Another goal is to prevent repeat attacks and long-term complications. Mayo Clinic notes that treatment may be needed for months to years in some cases. (Mayo Clinic)
If the cause is infectious, the infection must be treated directly. Depending on the diagnosis, that may mean antimicrobial, antiviral, antiparasitic, or antifungal therapy. Steroids may still play a role in controlling inflammation, but they are used carefully and usually alongside treatment for the infection rather than instead of it. (PMC)
If the cause is non-infectious, corticosteroids are commonly used to bring inflammation under control. These may be given as oral tablets, injections around the eye, injections inside the eye, or sometimes implants, depending on the case. Posterior disease usually cannot be controlled by standard eye drops alone because the problem is too far back in the eye. For patients who need longer-term control, steroid-sparing immunomodulatory medicines may be added to reduce repeated inflammation and limit steroid side effects. NIH notes that clinicians often use oral corticosteroids first for intermediate and posterior or panuveitis, then taper and move toward steroid-sparing therapy when appropriate. (National Institutes of Health (NIH))
Macular edema may need specific attention because even when the main inflammation seems quieter, swelling at the macula can continue to blur vision. OCT helps track this very closely. Sometimes patients are discouraged because the eye “looks better” but their vision has not fully returned. In these situations, persistent edema, retinal damage, or scarring may explain the slow improvement. (PMC)
What complications can happen if treatment is delayed?
The main danger is permanent loss of retinal function. Inflammation is not just irritation. It can leave structural damage behind. Posterior uveitis can lead to macular edema, retinal scarring, retinal detachment in some cases, optic nerve involvement, abnormal blood vessel changes, cataract, and glaucoma related either to the disease or to its treatment. The exact risk varies with the specific type of uveitis, how long it has been active, and how quickly it is controlled. (Moorfields Eye Hospital)
This is why I encourage patients not to judge seriousness by pain level alone. A mildly uncomfortable eye is not always less serious than a painful one. In posterior uveitis, the part of the eye that gives you sight is directly at risk. That is the central message patients and families need to understand. (Moorfields Eye Hospital)
Can it come back?
Yes, it can. Some cases are acute and settle well. Others are recurrent or chronic. The NIH and other expert sources emphasize that uveitis may return and sometimes requires long-term monitoring and treatment. Patients often feel relieved when symptoms improve, but follow-up remains important because inflammation can smolder again before obvious symptoms appear. (Mayo Clinic)
For that reason, successful care is not only about the first treatment. It is also about monitoring vision, scanning the retina, watching for medication side effects, and looking for relapse. Uveitis care can be a marathon, not a sprint. (Mayo Clinic)
When should you see a doctor urgently?
Please seek prompt eye care if you notice new floaters, a sudden drop in vision, a gray or blurry patch in your sight, increasing flashes, distortion, or any combination of blurred vision and eye inflammation symptoms. Even if the eye is not very red and does not hurt much, those symptoms deserve attention. Uveitis is one possibility, but there are other retinal emergencies that can sound similar, and those also need urgent assessment. (National Eye Institute)
If you already have a history of uveitis and your vision changes again, do not assume it will settle on its own. Recurrence is possible, and early review usually gives the best chance of limiting damage. (National Eye Institute)
Practical advice for patients and families
The most useful habit is to respect changes in vision, even when they seem mild. Cover one eye at a time and compare. If one eye is suddenly less clear, that matters. Keep a note of when symptoms began and whether floaters, haze, or missing spots are getting worse. Bring your medication list and any history of autoimmune disease, infection, or prior eye inflammation to the appointment. These details can help speed diagnosis. (National Eye Institute)
Do not self-treat a blurry eye with leftover steroid drops unless a doctor has told you exactly what to do. In posterior uveitis, drops alone may be inadequate, and in infectious cases unsupervised steroid use can be risky. (Mayo Clinic)
Final word
Posterior uveitis is a strong reminder that not all serious eye disease is noisy. Because it affects the retina and nearby tissues at the back of the eye, it may steal vision through blur, floaters, and swelling rather than through redness and pain. That quiet presentation is precisely why it deserves more awareness. If your sight is changing, especially with new floaters or unexplained blur, please do not wait for severe pain before seeking help. The retina does not need to hurt to be in danger. (Moorfields Eye Hospital)
If you are experiencing these symptoms, book an appointment with an ophthalmologist or retina specialist for a dilated eye examination and retinal imaging. Early treatment can make a real difference to the vision you keep. (National Eye Institute)
References
- American Academy of Ophthalmology — What Is Uveitis? (American Academy of Ophthalmology)
- National Eye Institute (NIH) — Uveitis (National Eye Institute)
- Mayo Clinic — Uveitis: Symptoms and causes (Mayo Clinic)
- Mayo Clinic — Uveitis: Diagnosis and treatment (Mayo Clinic)
- PMC review — Macular edema associated with non-infectious uveitis (PMC)





