
A droopy upper eyelid is not always “just tired eyes.” True ptosis is a change in eyelid position, and it may be present from birth or develop later because of aging, contact lens wear, surgery, nerve problems, muscle disease, swelling, or other illnesses. In children, severe ptosis can interfere with vision development and lead to amblyopia. In adults, sudden drooping, double vision, eye pain, headache, vomiting, or a change in pupil size needs urgent medical attention. A proper eye exam can tell whether you need observation, glasses, amblyopia treatment, or surgery. (American Academy of Ophthalmology)
Droopy Eyelid or Just Tired Eyes? The Ptosis Signs Indians Commonly Ignore
If you have ever searched “one eye not opening fully,” “eyelid feels heavy,” or “why does one eye look smaller in photos,” you are in very familiar company. In many Indian homes, a droopy eyelid is first blamed on lack of sleep, stress, mobile phone use, allergies, or “weakness.” Sometimes that is partly true. But sometimes the eyelid is not simply tired. It is actually drooping, and that has a name: ptosis.
As ophthalmologists, we see this confusion often. A patient says, “Doctor, my eye just looks sleepy.” A parent says, “My child has had this since birth, but she sees fine, so maybe it is only cosmetic.” Another person notices that one eyebrow is always raised in photographs, or that they lift the lid with a finger when reading. These are small clues, but they matter.
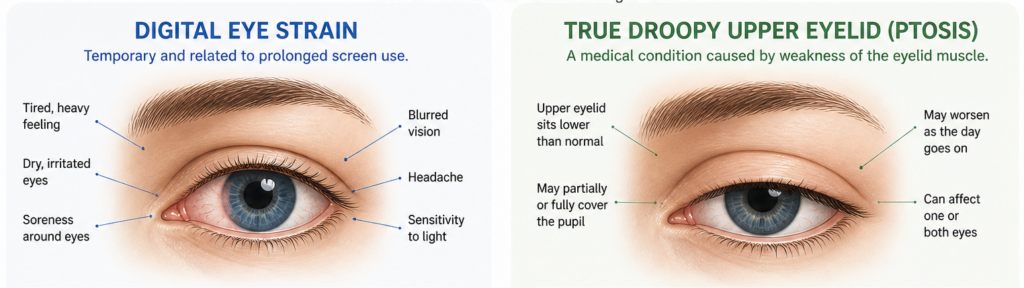
Ptosis means the upper eyelid sits lower than normal. It can be mild, where the lid only looks a little low, or severe, where it covers part of the pupil and blocks vision. It may affect one eye or both. In some people it is present from birth. In others it appears later because the eyelid-lifting muscle or its tendon has weakened, stretched, or been affected by a nerve or muscle problem. (American Academy of Ophthalmology)
Why ptosis gets mistaken for “tired eyes”
This is where the confusion begins. Ordinary eye strain from screen use can make the eyes feel tired, dry, blurry, or headachy. Digital eye strain is common with long periods of reading or mobile and computer use, and dry eye can also make the eyelids feel heavy. But these problems usually do not create a true, persistent change in the height of one upper eyelid. Ptosis, in contrast, is a position problem of the lid itself. (moorfields.nhs.uk)
A simple way to think about it is this: tired eyes are mostly about discomfort and visual fatigue; ptosis is about the lid sitting lower than it should. Of course, the two can exist together. Someone with ptosis may complain of tiredness because they are constantly using the forehead muscles to lift the lid. That effort can lead to brow ache, eye strain, and fatigue, especially during reading or concentration. (moorfields.nhs.uk)
The signs adults commonly ignore
The first overlooked sign is asymmetry. One eye looks smaller in photographs, especially in the evening or after a long workday. Sometimes the patient does not notice it, but relatives do. MedlinePlus notes that comparing current eyelid position with old photographs can help detect progression, and that is genuinely useful in clinic. (MedlinePlus)
The second sign is compensation. If you constantly raise one eyebrow, wrinkle your forehead, tilt your chin upward, or use a finger to lift the lid while reading, your body may be trying to work around a droopy eyelid. These are classic clues. They are easy to dismiss as habits, but they often tell us that the eyelid is interfering with the upper field of vision. (Cambridge University Hospitals)
The third sign is heaviness that is one-sided and visible. Many people say, “My eye feels heavy.” That phrase is important. If the heaviness is linked with a visibly lower lid, difficulty keeping the eyelid open, forehead strain, or increasing asymmetry, it deserves an eye exam. Moorfields specifically lists difficulty keeping the eyelids open, eyebrow ache, eyestrain, and fatigue among common ptosis symptoms. (moorfields.nhs.uk)
Another commonly ignored point is that not every acquired ptosis is simply age-related. In adults, ptosis often happens because the tendon connected to the eyelid-lifting muscle stretches with time. But it can also follow long-term contact lens wear, trauma, cataract surgery or other eye surgery, swelling of the lid, or less commonly a neurological or muscle disorder. (UH Sussex)
When “it gets worse in the evening” matters
This is a detail I never like patients to ignore. Some droopy lids fluctuate. They may look better in the morning and worse later in the day. When ptosis varies with activity and improves with rest, we begin thinking about muscle-related causes such as myasthenia gravis. MedlinePlus notes that drooping eyelids and double vision are among the most common first symptoms of myasthenia gravis, and that the weakness tends to worsen with activity and improve with rest. (MedlinePlus)
That does not mean every evening droop is myasthenia. Far from it. But a changing eyelid, especially if it comes with double vision, difficulty chewing, swallowing, speaking, holding the head up, or unusual fatigue, should not be brushed off as simple lack of sleep. (MedlinePlus)
The red flags that need urgent attention
Most ptosis is not an emergency. Some cases are slow, longstanding, and simply need routine evaluation. But sudden eyelid drooping is different. NHS guidance advises urgent assessment if an eyelid droops suddenly, if you cannot open or keep the eye open, or if the droop comes with eye pain, a very red eye, headache, nausea, vomiting, light sensitivity, or changes in vision. (nhs.uk)
There are a few combinations I want patients to remember clearly. A droopy eyelid plus double vision is urgent. A droopy eyelid plus headache or eye pain is urgent. A droopy eyelid plus a change in pupil size is urgent. MedlinePlus notes that third nerve palsy can cause ptosis, double vision, headache or eye pain, and an enlarged pupil. The AAO also warns that asymmetric ptosis can sometimes signal a serious underlying process needing urgent evaluation. (MedlinePlus)
If you develop a new droopy eyelid after trauma, along with severe redness, worsening vision, or new neurological symptoms, do not wait for it to “settle.” Seek urgent medical care. (nhs.uk)
What parents often miss in babies and children
This is the part many families underestimate. Congenital ptosis means the droopy eyelid is present from birth or becomes noticeable very early in life. In children, it is commonly due to poor development of the levator muscle, the muscle that lifts the eyelid. It can affect one eye or both. (AAPOS)
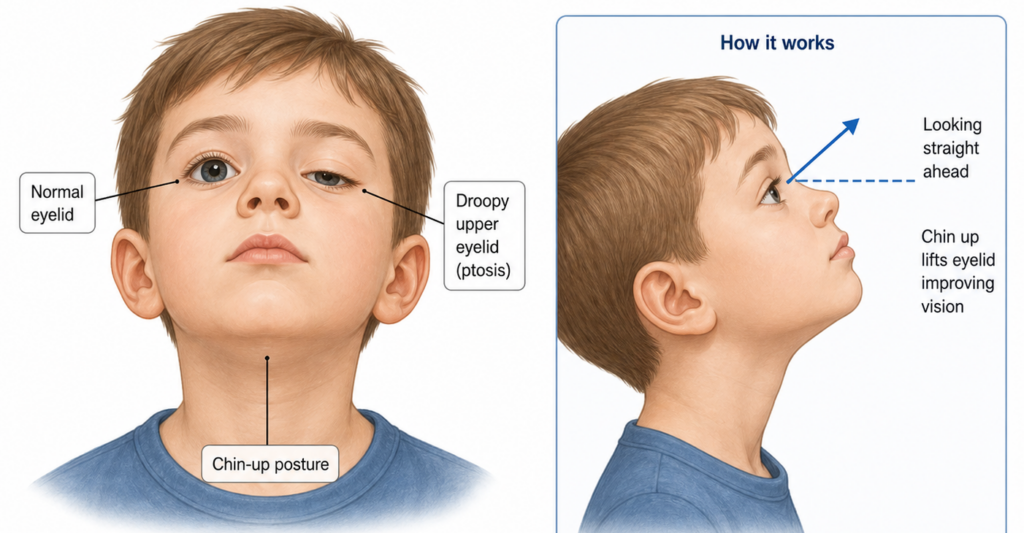
Parents often tell themselves, “He sees from underneath the lid, so maybe it is okay,” or “It runs in the family, so we are not worried.” That is understandable, but it is not always safe. A droopy lid can press on the eye and contribute to astigmatism, force a child into a chin-up head posture, or in more severe cases block the visual axis and interfere with normal visual development. That can lead to amblyopia, sometimes called lazy eye. (AAPOS)
AAPOS explains this very clearly: childhood ptosis may lead to astigmatism, abnormal head posture, and amblyopia. In rare severe cases, if the eyelid covers the eye completely, vision can fail to develop properly and permanent vision loss can occur. (AAPOS)
This is why every child with a droopy lid should be examined by an ophthalmologist, preferably one comfortable with pediatric eye disease. The goal is not only to look at the lid. It is to check vision, the need for glasses, head posture, amblyopia risk, and whether the pupil is being covered. (AAPOS)
Research also supports the concern. Published studies have found that congenital ptosis is associated with amblyopia, refractive errors, and strabismus, and one study reported an amblyopia incidence of 18% in children with moderate to severe congenital ptosis. (PMC)
Does every child need surgery immediately?
No. This is another common misunderstanding. Not every child with ptosis needs urgent surgery. If the droop is mild and vision is developing normally, careful follow-up may be enough for some time. AAPOS states that surgery is needed when the droopy lid causes vision problems that cannot be corrected with glasses or other treatment. Some NHS guidance notes that when vision is not threatened, surgery may be delayed until later childhood, often around the age when measurements are easier and facial growth is further along. (AAPOS)
But the opposite is also important: if the lid is covering the pupil, causing a significant chin-up posture, or contributing to poor visual development, waiting may be the wrong choice. Severe cases may need earlier intervention specifically to protect vision. (AAPOS)
How we diagnose ptosis in clinic
A proper evaluation is more detailed than many people expect. We look at eyelid position, how well the eyelid muscle works, whether the brow is helping too much, whether one pupil is different from the other, whether eye movements are normal, and whether the droopy lid is affecting the visual field. In children, we also assess vision development and the need for glasses. (AAPOS)
Sometimes no scans are needed at all. AAPOS notes that imaging such as CT or MRI is not always necessary. But if the story suggests a nerve problem, muscle disease, mass, or other unusual cause, additional tests may be required. Depending on the situation, doctors may order visual field testing, slit-lamp examination, blood tests for myasthenia gravis, or imaging. (AAPOS)
This is one reason self-diagnosis is risky. Not every “small eye” is ptosis. Sometimes there is excess eyelid skin rather than true muscle droop. Sometimes brow position changes the appearance. Sometimes swelling, a stye, allergy, or other lid disease makes the eyelid look different. And sometimes a droopy eyelid is part of a neurological condition. (MedlinePlus)
Treatment: observation, glasses, amblyopia care, or surgery
Treatment depends on the cause and on whether vision is at risk. Mild ptosis may only need observation and follow-up. If a disease is causing the droop, that condition must be treated. In children, treatment may also include glasses, patching, or atropine drops if amblyopia is present or developing. Surgery may be one part of the plan, not the whole plan. (UH Sussex)
When surgery is needed, the exact procedure depends on how well the eyelid muscle works. AAPOS describes two common approaches: levator resection, where the existing eyelid-lifting muscle is tightened if it still has some function, and frontalis sling, where the eyelid is linked to the forehead muscle if levator function is poor. (AAPOS)
In adults, surgery is usually considered when the droop significantly affects vision or function, though some people also seek treatment because the asymmetry is distressing. Surgical planning is based on measurements of the eyelid, muscle function, and visual field effect. (Cambridge University Hospitals)
What you should watch for at home
Before your appointment, do three simple things. First, look through older photos and note whether the droop is new or longstanding. Second, observe whether it is always present or changes during the day. Third, check for associated symptoms such as double vision, brow strain, chin-up posture, headache, eye pain, or a visibly different pupil. These details help your ophthalmologist sort harmless, age-related ptosis from more serious causes. (MedlinePlus)
For parents, watch whether the child tilts the head back, raises the eyebrows all the time, seems to look from under the lid, rubs one eye often, or resists visual tasks. Remember that children with amblyopia may not complain at all. Many do not realize one eye is seeing less clearly. (AAPOS)
When to see a specialist
If the droopy lid is longstanding and mild, book a routine ophthalmology visit. If it is affecting reading, driving, work, appearance, or confidence, it is still worth evaluating. If the patient is a child, do not postpone assessment simply because the eye “looks okay.” In childhood ptosis, the real question is not only how the eyelid looks today, but whether vision is developing normally. (MedlinePlus)
If the droop is sudden, rapidly worsening, associated with double vision, pupil change, eye pain, headache, nausea, vomiting, marked redness, or new visual symptoms, treat it as urgent. (nhs.uk)
A final word for Indian patients and parents
Please do not feel embarrassed if you have ignored this for months or years. That is common. Ptosis often looks subtle at first, and it is easy to blame tiredness, late nights, screens, or family resemblance. But a droopy upper eyelid is one of those signs that deserves a proper eye examination, especially in a child or when it is new in an adult.
If you or your child has a droopy eyelid, book an appointment with an ophthalmologist. In children, ask for pediatric ophthalmology assessment. In adults with significant lid droop, an oculoplasty-trained ophthalmologist may also be helpful. A careful exam can tell you whether this is harmless, whether vision is being affected, and whether you need monitoring or treatment.
References
- American Academy of Ophthalmology, “What Is Ptosis?” (American Academy of Ophthalmology)
- American Association for Pediatric Ophthalmology and Strabismus, “Ptosis.” (AAPOS)
- MedlinePlus, “Eyelid drooping.” (MedlinePlus)
- Moorfields Eye Hospital, “Ptosis (droopy eyelid).” (moorfields.nhs.uk)
- AAPOS, “Amblyopia.” (AAPOS)





