Recurring uveitis can be exhausting, especially when each flare seems to trigger more blood tests, scans, and specialist visits without a clear answer. That does happen. Many cases are still labeled idiopathic, which means no definite cause has been found yet, not that the symptoms are “in your head.” Specialists usually escalate step by step: first confirming the inflammation pattern, then ruling out important infections and autoimmune diseases, then using imaging, targeted lab work, and sometimes systemic treatment or referral to rheumatology, retina, or infectious disease when flares keep returning or threaten vision.
Recurring Uveitis With No Clear Cause: What Tests Patients Keep Getting and When Specialists Escalate Care
When a patient says, “My eye keeps flaring up, but nobody can tell me why,” I understand the frustration. Recurrent uveitis is one of the most emotionally draining eye problems because the inflammation is real, the symptoms are disruptive, and yet the explanation may remain unclear for months or even years. Uveitis is inflammation inside the eye. It can cause pain, redness, light sensitivity, floaters, blurred vision, and sometimes permanent vision loss if not treated promptly. It may affect one eye or both, and it can appear as a single event, as repeated flares, or as chronic ongoing inflammation. (National Eye Institute)
A point that helps many patients is this: “idiopathic” does not mean the doctor has stopped caring or believes nothing is wrong. It simply means that, even after evaluation, no definite trigger has been proven. According to major ophthalmology references, many uveitis cases are idiopathic, and the likelihood of finding a cause depends partly on where the inflammation is located in the eye and what the examination looks like. Anterior uveitis, intermediate uveitis, posterior uveitis, and panuveitis can each point toward different causes and different workups. (Merck Manuals)
Why doctors do not always find a root cause right away
Patients often expect one decisive test, like a single blood marker, MRI, or scan that will explain everything. Unfortunately, uveitis rarely works that way. Diagnosis begins with the eye exam, not the lab slip. A specialist first tries to answer several clinical questions: Which part of the eye is inflamed? Is the flare acute or chronic? Is it unilateral or bilateral? Does it look granulomatous or nongranulomatous? Are there retinal lesions, vascular changes, macular edema, high eye pressure, or signs suggesting an infection such as herpes, toxoplasmosis, tuberculosis, or syphilis? The exam helps decide which tests are worth ordering and which would probably create noise rather than answers. (Merck Manuals)
This is why one specialist may order a compact, targeted set of tests while another may repeat a few studies later. It is not always duplication for its own sake. Sometimes the pattern has changed. Sometimes previous results are outdated, incomplete, or unavailable. Sometimes treatment decisions now carry more weight, especially if the team is considering steroid-sparing immunosuppressive therapy, biologic treatment, or referral outside ophthalmology. In recurrent disease, doctors are often balancing two tasks at once: calming the eye and continuing to look for an underlying condition that would change long-term management. (American Academy of Ophthalmology)
The tests patients commonly keep getting
The first and most important “test” is usually the detailed ophthalmic examination. That includes a slit-lamp exam, a pressure check, and a dilated examination of the back of the eye. These steps help confirm whether the problem is truly uveitis and not something that can mimic it, such as keratitis, scleritis, angle-closure glaucoma, or, more rarely, an intraocular tumor or lymphoma. In other words, before escalating the medical workup, specialists need to be sure they are treating the right disease. (Merck Manuals)
After that, the next wave of testing is often blood work and selected imaging. One commonly cited AAO approach emphasizes “smart choices” rather than blanket testing of every possible autoimmune marker. In many recurrent anterior uveitis cases, specialists consider tests such as HLA-B27 and syphilis serology. If the examination suggests sarcoidosis or tuberculosis, chest imaging and tests such as serum ACE, lysozyme, and TB screening may be added, though the exact combination varies among clinicians and practice settings. (American Academy of Ophthalmology)
That explains why patients frequently remember repeating some version of the following:
HLA-B27 testing, especially when flares are recurrent, painful, sudden, or linked with back pain, joint stiffness, psoriasis, or bowel disease. HLA-B27 can be associated with spondyloarthropathies and recurrent acute anterior uveitis. (Merck Manuals)
Syphilis testing, often with treponemal and nontreponemal blood tests. Syphilis is a classic “must not miss” cause because it can imitate many ocular inflammatory patterns and because identifying it changes treatment completely. (Merck Manuals)
Tuberculosis screening, often with an interferon-gamma release assay such as QuantiFERON or a skin test, sometimes paired with chest imaging. TB becomes more relevant if the person has risk factors, compatible eye findings, or comes from or has traveled to a region with higher prevalence. (Merck Manuals)
Sarcoidosis-related testing, which may include a chest X-ray or chest CT and selected blood tests. Sarcoidosis can affect the lungs and lymph nodes as well as the eyes, and some patterns of bilateral or granulomatous inflammation make doctors look more closely for it. (Merck Manuals)
Inflammatory or autoimmune screening, sometimes including ANA, rheumatoid factor, ANCA, ESR, or CRP. These tests are not equally useful in all adults with uveitis, which is why many uveitis specialists avoid ordering them reflexively unless the history or exam points in that direction. (American Academy of Ophthalmology)
Viral or infectious testing, especially if the flare is one-sided, associated with high pressure, iris changes, retinal scars, or an appearance that raises concern for herpes-family infection, toxoplasmosis, or other infection. (Merck Manuals)
Why some labs get repeated
Repeated labs are one of the biggest sources of patient annoyance. There are several reasons this happens. First, some tests are screening tools, not final answers. A borderline result may need confirmation. Second, a test done years ago may not be enough when the disease pattern has changed or when immunosuppression is being considered. Third, results performed at another hospital may not be easy to access or may not have included the exact assay now needed. Fourth, infectious evaluations often need to be current before escalating immune-suppressing treatment, because suppressing the immune system in someone with untreated infection can be dangerous. (American Academy of Ophthalmology)
It is also common for patients to hear, “Your blood work is normal,” and feel that the evaluation has failed. In reality, normal blood work is still useful. It can lower the suspicion for certain diseases and help doctors choose safer next steps. The challenge is that many uveitis-associated conditions do not show up neatly on broad screening panels, and some patients with true immune-mediated eye disease still have largely normal routine blood tests. That is one reason the eye findings themselves remain central to decision-making. (American Academy of Ophthalmology)
The scans and eye imaging specialists use as care escalates
Many patients think of lab tests first, but eye imaging often becomes more important over time. If recurrent uveitis is affecting the back of the eye, causing floaters, reducing vision, or raising concern for macular edema, your specialist may order optical coherence tomography, commonly called OCT. OCT gives a cross-sectional view of the retina and is especially helpful for detecting and monitoring macular swelling, which is one of the most common reasons vision drops in uveitis. (Merck Manuals)
Fluorescein angiography may be used when doctors need to look for leakage from retinal blood vessels, optic nerve inflammation, vasculitis, or macular edema that is not obvious on routine examination. This test becomes more likely when the disease is intermediate, posterior, or panuveitic, or when vision seems worse than the front-of-eye findings alone would explain. (EyeWiki)
Other imaging may include fundus photography, widefield imaging, B-scan ultrasound if the view into the eye is poor, or occasionally OCT angiography in selected settings. These are not “extra” tests ordered just to be thorough. They help define whether inflammation is active, whether damage is accumulating, and whether treatment is working. That information often matters more than another round of broad autoimmune blood work. (EyeWiki)
When a general ophthalmologist refers to a uveitis specialist
Escalation often begins with referral. A general ophthalmologist may manage a simple first episode of anterior uveitis, but recurrent disease usually raises the threshold for subspecialty input. Referral becomes more likely when flares keep returning, the inflammation is hard to control, steroid side effects are developing, both eyes are involved, the back of the eye is affected, the diagnosis is uncertain, or the patient might need long-term immune-modifying treatment. (Merck Manuals)
A uveitis specialist typically narrows the pattern more precisely. That may lead to fewer random tests and more focused ones. Sometimes the biggest change is not the number of tests but the interpretation of the whole picture. Two patients may both have “recurrent uveitis,” but one may really fit HLA-B27-associated disease, another sarcoid-type inflammation, another a viral hypertensive uveitis, and another a masquerade syndrome that needs a different pathway entirely. (Merck Manuals)
When care escalates beyond ophthalmology
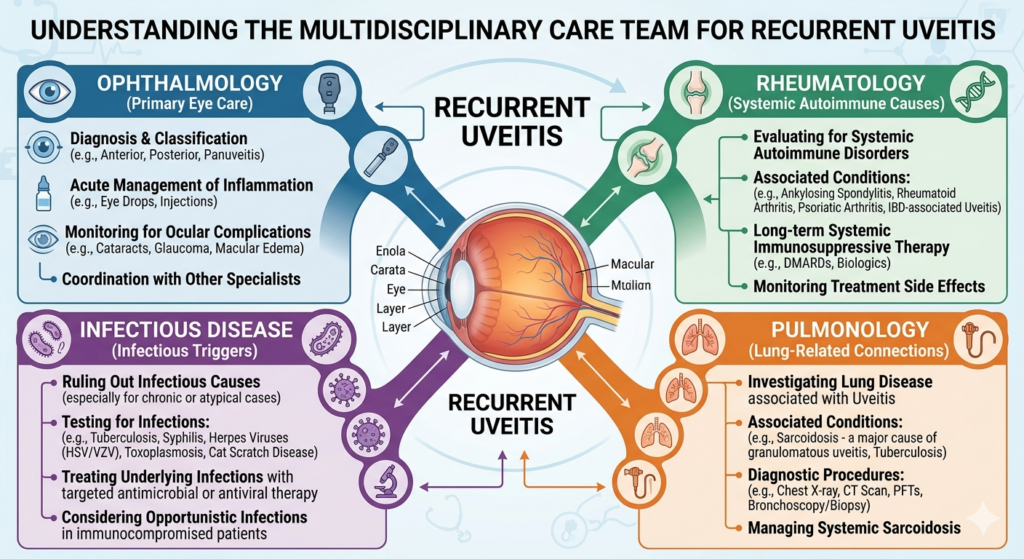
Many patients wonder why they are suddenly being sent to rheumatology, infectious disease, pulmonology, neurology, or even nephrology. This usually happens because the eye findings suggest that the uveitis is part of a larger systemic disease, or because treatment decisions now affect the whole body.
Rheumatology referral is common when there are signs of inflammatory arthritis, psoriasis, bowel disease, juvenile idiopathic arthritis, or when noninfectious uveitis may require steroid-sparing systemic treatment such as methotrexate, mycophenolate, or biologic therapy. These medications can protect vision, but they require systemic review and monitoring. (Merck Manuals)
Infectious disease referral may happen when syphilis, tuberculosis, herpes-family infection, toxoplasmosis, or another infection is suspected or confirmed. This is especially important because the treatment direction changes completely. Infectious uveitis is not managed the same way as autoimmune uveitis, and steroids alone may be unsafe in some infectious settings. (Merck Manuals)
Pulmonology may become involved if chest imaging suggests sarcoidosis or TB. Neurology may be involved if intermediate uveitis raises concern for multiple sclerosis or if symptoms such as numbness, weakness, or neurological episodes are present. Nephrology may enter the picture if tubulointerstitial nephritis and uveitis syndrome is suspected. Again, this does not mean doctors are starting over. It means the eye is acting as a clue to a bigger diagnosis. (Merck Manuals)
When treatment escalation becomes necessary
Patients often recognize escalation not by the tests, but by the medicines. Early flares are often treated with steroid eye drops and cycloplegic drops to calm inflammation and pain. That is standard, especially for anterior uveitis. But repeated steroid courses are not harmless. Long-term or repeated steroid use can contribute to cataract and glaucoma, and uncontrolled uveitis itself can also damage the eye. (Merck Manuals)
That is why specialists begin talking about escalation when any of the following happen: flares become frequent, inflammation returns quickly during steroid taper, both eyes are involved, the posterior segment is affected, OCT shows macular edema, vision is worsening, or steroid side effects are appearing. At that point, local steroid injections, steroid implants, oral steroids, or steroid-sparing immunosuppressive medications may be considered depending on the cause and location of inflammation. (Merck Manuals)
For selected adults with noninfectious posterior segment uveitis, NICE guidance supports adalimumab in people with active disease, inadequate response or intolerance to immunosuppressants, systemic disease or bilateral involvement, and worsening vision with a high risk of blindness. Dexamethasone intravitreal implant is also recommended in certain adults with active disease and worsening vision with risk of blindness. These are not first-line choices for every patient, but they show what escalation can look like when recurrent inflammation is vision-threatening. (NICE)
What patients should ask when the workup feels endless
When the same testing cycle keeps repeating, patients deserve a clearer roadmap. Helpful questions include: What pattern of uveitis do I have? Which diagnoses are still on the table? Which infections have been ruled out? Are we repeating this test because the result may have changed, because it was incomplete, or because it affects the next treatment step? Is this still considered idiopathic, or do you suspect a syndrome even without full proof? Do I need a uveitis specialist, retina specialist, or rheumatologist now? Those questions can turn a confusing workup into a more understandable plan. (American Academy of Ophthalmology)
It also helps to keep your own flare diary. Note which eye was affected, the date, symptoms, drop schedule, response to treatment, associated illnesses, joint pain, skin rash, mouth ulcers, bowel symptoms, fevers, travel, infections, or new medications. A pattern that seems invisible in one visit may become obvious over six or twelve months. This kind of history can be more useful than another broad lab panel. That is not a formal guideline statement, but it is a practical truth in recurrent inflammatory disease.
When to seek urgent care
Any new or recurrent flare deserves prompt ophthalmic assessment. National guidance emphasizes urgent eye review for suspected uveitis because delayed treatment can risk vision. Sudden pain, marked light sensitivity, decreased vision, a shower of new floaters, or redness with blur should not be watched at home for days. Recurrent disease can sometimes feel “familiar,” but even familiar flares can behave differently and lead to new complications such as macular edema, glaucoma, or retinal problems. (NICE CKS)
The emotional side of “no clear cause”
One of the hardest parts of recurrent uveitis is feeling stuck between two unsatisfying truths: the disease is serious, yet the cause may still be uncertain. Patients may begin to worry that they are missing a hidden infection, a cancer, or a major autoimmune disorder. Sometimes those fears are appropriate to investigate, but often the more realistic answer is that uveitis is a heterogeneous group of diseases and not every case yields a neat label. The goal of specialist care is not only naming the disease. It is protecting vision, ruling out dangerous treatable causes, and escalating therapy when the eye needs more than repeated rescue treatment. (Merck Manuals)
So if you have been told your recurrent uveitis is idiopathic, do not hear that as dismissal. Hear it as a staging point. The evaluation may still evolve. A clue may emerge later. But even before a root cause is found, good care can still be very active, thoughtful, and effective.

When to See a Doctor
You should contact an ophthalmologist urgently if you develop eye pain, light sensitivity, redness, blurred vision, or new floaters, especially if you have had uveitis before. You should also seek prompt review if your symptoms are recurring during a steroid taper, if you are needing frequent steroid drops, or if another doctor has suggested that treatment may need to move beyond drops. Recurrent uveitis is exactly the kind of problem where early specialist review can prevent avoidable damage. (National Eye Institute)
Call to Action
If you are experiencing repeated uveitis flares without a clear explanation, book an appointment with a uveitis-trained ophthalmologist or an eye hospital that can coordinate retina, rheumatology, and infectious disease input when needed. A structured review of your flare pattern, prior test results, and imaging can often clarify whether you need more testing, a different diagnosis pathway, or a stronger long-term treatment plan.
References
- National Eye Institute. Uveitis. (National Eye Institute)
- Merck Manual Professional Edition. Overview of Uveitis. (Merck Manuals)
- American Academy of Ophthalmology. Uveitis Laboratory Work Up: Making Smart Choices. (American Academy of Ophthalmology)
- NICE. Adalimumab and dexamethasone for treating non-infectious uveitis. (NICE)
- American Academy of Ophthalmology. Acute Anterior Uveitis. (EyeWiki)